GMJ Medicine
eISSN : 2626-3041

Embase

Biosis Previews
description
Volume 2, Issue 2 (2023)
GMJM 2023, 2(2): 51-56 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2022/10/3 | Accepted: 2023/03/22 | Published: 2023/05/12
Received: 2022/10/3 | Accepted: 2023/03/22 | Published: 2023/05/12
How to cite this article
Milani Fard M. Laboratory Findings of Bacterial Meningitis in Children. GMJM 2023; 2 (2) :51-56
URL: http://gmedicine.de/article-2-189-en.html
URL: http://gmedicine.de/article-2-189-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

Authors
M. Milani Fard *
Department of Anatomy, Faculty of Medicine, Iran University of Medical Sciences, Tehran, Iran
Keywords:
| Abstract (HTML) (1731 Views)
Full-Text: (602 Views)
Introduction
In meningitis, seconds and minutes are very important and should be diagnosed as soon as possible and treatment started as soon as possible. A patient after clinical diagnosis of meningitis or high suspicion of it and an overview of the possible source of infection (ear, sinuses, urinary tract, skin…) should be taken immediately in the absence of local neurological signs and symptoms and Papular edema to take cerebrospinal fluid. But if there is a neurological disorder, you must first have a CT scan to rule out space-occupying lesions in the brain. The scan was performed and if it was negative, then proceeded to LP (Figure 1).
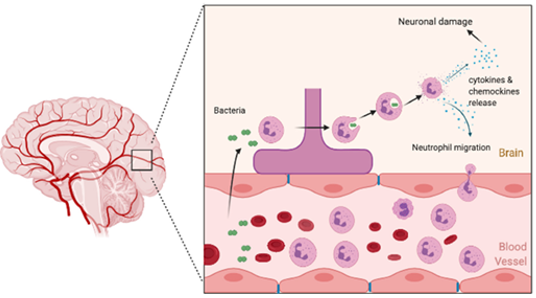
Figure 1) Bacterial meningitis in children
Given the tremendous importance of meningitis in pediatrics and the key role that diagnostic tests play in identifying this deadly disease, and given that many diagnostic tests available in our country are far from reaching world standards (e.g. In pediatric meningitis, CSF culture rarely yields acceptable results. We decided to first evaluate the diagnostic value of each of the clinical signs of meningitis and identify the most common manifestations of meningitis in our country. Therefore, we should evaluate the diagnostic value of laboratory diagnostic tests in patients with proven meningitis and briefly explain to an Iranian physician how much he can trust the patient's symptoms and how much he can rely on laboratory results. Trust. Also, in another part of this plan, common objects involving the CNS (in the form of meningitis) will be identified, which will greatly help in the choice of experimental treatment in these patients. Complications of meningitis are divided into unstable and stable groups: Unstable complications include: subdural effusion, ADH, prolonged fever (Figure 2). Permanent complications include: neurological disorders, mental retardation, seizures, learning disabilities, visual impairment, behavioral disorders [1-15].
When the skull is broken by an accident such as an accident, the same pieces of bone may tear the meningeal layers, and if tissue repair is not done properly, it may cause meningitis. Meningitis is a protective layer on the brain and spinal cord, so if someone has meningitis or inflammation of the meninges, it must be determined that the meningitis is of spinal or cerebral origin [16-22].
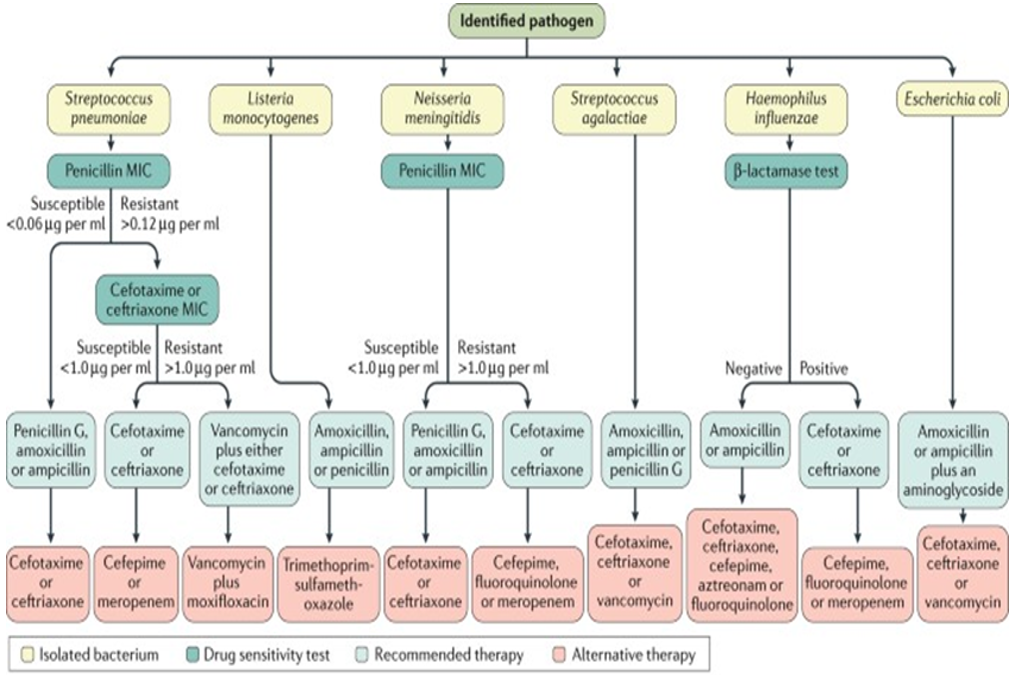
Figure 2) Community-acquired bacterial meningitis
If germs or foreign matter enter the fluid through the blood vessels in any way and cause infection, the bones that protect the meninges will break and cause tissue damage, or any other factor that can cause inflammation of these membranes can occur. Give meningitis in the brain or spinal cord. Most people consider meningitis to be an infection due to insufficient information, but this is not always the case.
The inflammatory source of meningitis is often viral or bacterial and should be treated as soon as the disease is known. The type of treatment and even its severity varies depending on the underlying cause of meningitis. In some people, the disease can be cured even without treatment and only with supportive therapies, but in others, for example, if the invasive agent is the herpes simplex virus, more specific treatment is needed [23-30]. In addition, bacterial meningitis is much more dangerous and requires immediate action. The patient must be treated correctly and based on the underlying cause of the inflammation. If treated incorrectly, the patient may progress to coma or even death.
Bacteria are an important and common cause of meningitis and may enter the nerve or cerebrospinal fluid in different ways. For example, a person who has had a bedsore or even had an infection, apse, or wound in other parts of his body has also developed meningitis. Bacteria that enter the bloodstream and enter the brain and spinal cord along the way cause acute bacterial meningitis. In most cases, the bacteria enter the bloodstream during an infection and contaminate the blood or, in scientific terms, cause sepsis and bacteremia. The bacterium then enters other tissues, such as nerve tissue, during the vascular exchange [31-37]. For example:
• During surgery with contaminated equipment or even at the dentist, if poor quality equipment is used, the bacteria can spread to other parts of the nervous system through the blood or nerve of the tooth.
• During accidents and bone fractures, the infectious agent can enter directly from the damaged scalp.
• During the LP or Lumbar Puncture, in which the doctor inserts a needle into the area to sample cerebrospinal fluid (CSF), the bacteria can enter the meningeal fluid directly if the equipment is contaminated during this invasive procedure.
• Even dental infections that spread to the ear and infections that start in the ear themselves can be transmitted to the auditory nerve or balance due to neglect and open their way to the brain and spinal cord.
Instrument and Methods
In this retrospective cross-sectional study in 2019-2021, a total of 122 patients were selected randomly by referring to the archives of Fatemi Children's Hospital, Qom Stock Exchange, Iran.
With a diagnosis of bacterial meningitis in the files of hospitalized children, age, sex, the reason for referral, blood sugar, number of blood leukocytes, blood BUN, blood Cr, blood Na+ blood, K+ blood, blood culture positive, number of CSF leukocytes, glc in CSF, Pr in CSF, CSF Culture positivedata were collected using a checklist..
In the CSF, cell count and protein differentiation, protein level, glucose level are checked and hot staining, bacterial culture, and in cases of suspected Cryptococcus, fungal culture and agglutination, and latex tests are performed to check for polysaccharide Buccal antigens.
By collecting information and classifying and separating them and using the SPSS 20 software package, the information was analyzed.
Findings
A total of 122 patients were analyzed, of which 50 were girls (41%) and 72 were boys (59%). The ratio of boys to girls is 1.43 to 1. 19 patients (15.9%) were in the age group under 2 months and 69 patients (56.6%) were in the age group of 2 months to the end of 7 years and 43 patients (27.9%) were also in the age group over 7 years. Out of 19 people under 2 months of age, 4 (21.1%) were girls and 15 (78.9%) were boys. Of 69 people in the age group of 2 months to 7 years, 31 (44.9%) were girls and 38 (55.1%) were boys and out of 34 people in the age group over 7 years, 15 (44.1%) were girls and 19 (55.9%) were boys. In 106 (86.9%) of these patients, fever was mentioned as one of the reasons for referral. Nausea in 75 patients (61.5%) was one of the causes of referral. Vomiting in 80 patients (65.6%), headache in 52 patients (42.6%), cough in 11 patients (9%), restlessness in 6 patients (4.9%), seizures in 8 patients (6.6%), lethargy in 23 patients (18.9%) and not breastfeeding and anorexia in 10 patients (8.2%) were the main complaints. In the age group under 2 months, fever was the most common reason for hospitalization in 68.4%, followed by non-breastfeeding in 36.8%, restlessness and lethargy in 21.1% of patients, and vomiting and seizures in 5.3% of patients. Has been the most common reason for hospitalization. Vomiting, nausea in 47 patients (68.1%), headache in 26 patients (37.7%), nausea in 15 patients (21.7%)
Indifference and cough were the most common causes in 10 patients (14.5%). In the age group over 7 years, the most common reasons for hospitalization were as follows: fever 9 (85.3%), nausea and vomiting 28 (82.4%), headache 26 (76.5%), lethargy 4 People (11.8%), Seizures were observed in 2 patients (5.9%) and cough in 1 patient (2.9%). In the study of blood glucose, the mean hospital stay time in the under 2 months group was 93.42. (Standard deviation 58.67) with a minimum of 29 and a maximum of 251. In the age group of 2 months to the end of 7 years, the mean blood sugar at the time of admission (39.36) was 11.25 with a minimum of 46 and a maximum of 217.
In the age group over 7 years, the mean blood glucose at the time of admission (43.71) was 122.68, with a minimum of 78 and a maximum of 256. In total, only 2 people had hypoglycemia in the age group under 2 months. Of the total number of children, 45 (36.8%) had leukocytosis, of which 2 (16.7%) in the age group under 2 months, 28 (40.6%) in the age group of 2 months to 7 years, and 15 people (44.1%) were in the age group over 7 years. The mean levels of BUN and Cr in the group of children under 2 months are 29.78 (14.6) and 1.24 (2.2), respectively, while in the age group of 2 months to 7 years, these values are respectively (9.9). 17) 25.98 and (65%) 0.66 and in the age group over 7 years are 27.35 (9.4) and 0.64 (17%), respectively.
In the total population of children studied, an increase in BUN in 57 cases (46.7%) was identified, of which 12 (66.7%) in the age group under 2 months, 28 (53.8%) in the age group 2 months to 7 years old and 17 people (65.4%) were in the group of children over 7 years old. Cr level increased in 28 children (22.9%) of which 15 (83.3%) were under 2 months old, 8 (16%) were 2 months to 7 years old and 5 (20%) They are in the age group over 7 years. In the study of electrolytes, the mean level of Na+ in the age group up to 2 months (4.7) was 139.38, in the age group 2 months to 7 years (5.4) 133.61, and in the age group over 7 years (6) 134.81 Was. There were 47 cases (38.5%) in the total population of Hyponatremia, of which 4 cases (3.8%) in the age group under 2 months, 30 cases (58.8%) in the age group 2 months to 7 years, and 13 cases (50%) were over 7 years old in the age group. The mean level of K+ in the age group up to 2 months (84%) was 5.13, in the age group 2 months to 7 years (88%) was 4.13 and in the age group over 7 years (51%) was 3.85. There were 16 cases of hypokalemia, of which 10 patients (19.6%) were in the age group of 2 months to 7 years and 6 patients (235.1) were in the age group over 7 years. In the study of blood culture test results, 188 cases were reported to be negative (96.7%) and 4 cases (3.27%) were reported as positive, including one case of Citrobacter, one case of Pneumococcus, one case of Sod and Mona, and one case of Staphylococcus.
Discussion
Based on the data, we conclude that bacterial meningitis is more common in boys than girls and is most common between the ages of 2 months and 7 years. In the paper, it is mentioned that purulent meningitis is more common in boys than girls. It is most common between the ages of 2 months and 2 years. In the clinical picture, fever was the most common reason for referral. After fever, nausea, restlessness, and lethargy were the most common symptoms in the age group under 2 months, and nausea, vomiting, and headache after fever were the most common symptoms in the two age groups. These results are consistent with the sources mentioned in irritants, restlessness, and non-breastfeeding are significant in young infants and there is usually fever. Older children may experience disturbances of consciousness and back pain, and usually have Corning and Brodsky symptoms if they are diagnosed with bacterial meningitis. Seizures and coma may occur. Elsewhere, acute central nervous system infection is the most common cause of fever along with signs and symptoms of central nervous system disease in children. There were extensive changes in the blood glucose at the time of referral, but the mean blood sugar in all three groups was in the normal range and only two patients had hypoglycemia, which was in the age group of fewer than 2 months, which was probably due to not breastfeeding. The presence of leukocytosis in the age group under 2 months was not a suitable indicator for the diagnosis of bacterial meningitis, while in the two age groups over 2 months, about half of the patients had clear leukocytosis [38].
It is noteworthy that in 101 patients (82.7%) the number of neutrophils constitutes 50% of the number of WBCs, of which 17 (89.7%) in the age group under 2 months, 58 (84%) in the group 2 months to 7 years old and 26 people (76.4%) are in the age group over 7 years. References in the diagnosis of bacterial meningitis do not mention WBC in the blood because the main criterion for diagnosis is based on CSF fluid analysis. The mean levels of BUN and Cr in the age group under 2 months were in the range higher than normal, but in the other two age groups, the mean levels of BUN and Cr were in the acceptable range. In this case, no similar study was performed.
Hyponatremia and hypokalemia are relatively common in the age group above 2 months, while in the age group under 2 months these electrolytes were in the normal range. Hypokalemia is not mentioned in the literature, but Hyponatremia is considered very important due to the syndrome of disproportionate secretion of antidiuretic hormone (SIADH), which causes excessive fluid retention and increases the risk of intracranial pressure. The amount of fluid therapy plays an important role. The incidence of this syndrome has been determined in 30-50% of patients.
The value of blood culture was very weak in confirming the diagnosis of meningitis because no information was recorded for 64 cases (52.4%) and on the other hand in other cases (44.2%) 54 cases were negative and only (3.27%) positive cases have been mentioned. According to blood culture sources, it is positive in 50-90% of patients.
In the study of CSF leukocytes, we concluded that this variable has a high diagnostic value, and this value increases with age, so that in the age group over 7 years, 100% of leukocytes have increased, and in the same study, this We found that in 87.7% of cases neutrophils constitute more than 50% of CSF leukocytes. However, in 2.4% of cases, we did not have information about the percentage of CSF neutrophils. In the remaining 9.9% of cases, they were either TB meningitis or had a positive culture and smear, or the diagnosis was based solely on response to treatment.
Sources also state that in acute bacterial meningitis the number of WBCs in CSF is 60000-100 and elsewhere it is 1000-100 that PMNs often form. In poorly treated bacterial meningitis, the number is 1-1000, and elsewhere is 5-10000, where PMNs are usually predominant, but if the treatment is prolonged, mononuclear cells are predominant. In Tuberculous meningitis, there are 10-500, which are mostly Polymorphonuclear and then mostly lymphocytes and monocytes.
Conclusion
Bacterial meningitis is more common in boys than girls and is more common in the age group of 2 months to 7 years than in other ages. The most common cause is fever.
Acknowledgements: None declared by the authors.
Ethical Permission: None declared by the authors.
Conflicts of Interests: None declared by the authors.
Funding/Support: None declared by the authors.
In meningitis, seconds and minutes are very important and should be diagnosed as soon as possible and treatment started as soon as possible. A patient after clinical diagnosis of meningitis or high suspicion of it and an overview of the possible source of infection (ear, sinuses, urinary tract, skin…) should be taken immediately in the absence of local neurological signs and symptoms and Papular edema to take cerebrospinal fluid. But if there is a neurological disorder, you must first have a CT scan to rule out space-occupying lesions in the brain. The scan was performed and if it was negative, then proceeded to LP (Figure 1).
Figure 1) Bacterial meningitis in children
Given the tremendous importance of meningitis in pediatrics and the key role that diagnostic tests play in identifying this deadly disease, and given that many diagnostic tests available in our country are far from reaching world standards (e.g. In pediatric meningitis, CSF culture rarely yields acceptable results. We decided to first evaluate the diagnostic value of each of the clinical signs of meningitis and identify the most common manifestations of meningitis in our country. Therefore, we should evaluate the diagnostic value of laboratory diagnostic tests in patients with proven meningitis and briefly explain to an Iranian physician how much he can trust the patient's symptoms and how much he can rely on laboratory results. Trust. Also, in another part of this plan, common objects involving the CNS (in the form of meningitis) will be identified, which will greatly help in the choice of experimental treatment in these patients. Complications of meningitis are divided into unstable and stable groups: Unstable complications include: subdural effusion, ADH, prolonged fever (Figure 2). Permanent complications include: neurological disorders, mental retardation, seizures, learning disabilities, visual impairment, behavioral disorders [1-15].
When the skull is broken by an accident such as an accident, the same pieces of bone may tear the meningeal layers, and if tissue repair is not done properly, it may cause meningitis. Meningitis is a protective layer on the brain and spinal cord, so if someone has meningitis or inflammation of the meninges, it must be determined that the meningitis is of spinal or cerebral origin [16-22].
Figure 2) Community-acquired bacterial meningitis
If germs or foreign matter enter the fluid through the blood vessels in any way and cause infection, the bones that protect the meninges will break and cause tissue damage, or any other factor that can cause inflammation of these membranes can occur. Give meningitis in the brain or spinal cord. Most people consider meningitis to be an infection due to insufficient information, but this is not always the case.
The inflammatory source of meningitis is often viral or bacterial and should be treated as soon as the disease is known. The type of treatment and even its severity varies depending on the underlying cause of meningitis. In some people, the disease can be cured even without treatment and only with supportive therapies, but in others, for example, if the invasive agent is the herpes simplex virus, more specific treatment is needed [23-30]. In addition, bacterial meningitis is much more dangerous and requires immediate action. The patient must be treated correctly and based on the underlying cause of the inflammation. If treated incorrectly, the patient may progress to coma or even death.
Bacteria are an important and common cause of meningitis and may enter the nerve or cerebrospinal fluid in different ways. For example, a person who has had a bedsore or even had an infection, apse, or wound in other parts of his body has also developed meningitis. Bacteria that enter the bloodstream and enter the brain and spinal cord along the way cause acute bacterial meningitis. In most cases, the bacteria enter the bloodstream during an infection and contaminate the blood or, in scientific terms, cause sepsis and bacteremia. The bacterium then enters other tissues, such as nerve tissue, during the vascular exchange [31-37]. For example:
• During surgery with contaminated equipment or even at the dentist, if poor quality equipment is used, the bacteria can spread to other parts of the nervous system through the blood or nerve of the tooth.
• During accidents and bone fractures, the infectious agent can enter directly from the damaged scalp.
• During the LP or Lumbar Puncture, in which the doctor inserts a needle into the area to sample cerebrospinal fluid (CSF), the bacteria can enter the meningeal fluid directly if the equipment is contaminated during this invasive procedure.
• Even dental infections that spread to the ear and infections that start in the ear themselves can be transmitted to the auditory nerve or balance due to neglect and open their way to the brain and spinal cord.
Instrument and Methods
In this retrospective cross-sectional study in 2019-2021, a total of 122 patients were selected randomly by referring to the archives of Fatemi Children's Hospital, Qom Stock Exchange, Iran.
With a diagnosis of bacterial meningitis in the files of hospitalized children, age, sex, the reason for referral, blood sugar, number of blood leukocytes, blood BUN, blood Cr, blood Na+ blood, K+ blood, blood culture positive, number of CSF leukocytes, glc in CSF, Pr in CSF, CSF Culture positivedata were collected using a checklist..
In the CSF, cell count and protein differentiation, protein level, glucose level are checked and hot staining, bacterial culture, and in cases of suspected Cryptococcus, fungal culture and agglutination, and latex tests are performed to check for polysaccharide Buccal antigens.
By collecting information and classifying and separating them and using the SPSS 20 software package, the information was analyzed.
Findings
A total of 122 patients were analyzed, of which 50 were girls (41%) and 72 were boys (59%). The ratio of boys to girls is 1.43 to 1. 19 patients (15.9%) were in the age group under 2 months and 69 patients (56.6%) were in the age group of 2 months to the end of 7 years and 43 patients (27.9%) were also in the age group over 7 years. Out of 19 people under 2 months of age, 4 (21.1%) were girls and 15 (78.9%) were boys. Of 69 people in the age group of 2 months to 7 years, 31 (44.9%) were girls and 38 (55.1%) were boys and out of 34 people in the age group over 7 years, 15 (44.1%) were girls and 19 (55.9%) were boys. In 106 (86.9%) of these patients, fever was mentioned as one of the reasons for referral. Nausea in 75 patients (61.5%) was one of the causes of referral. Vomiting in 80 patients (65.6%), headache in 52 patients (42.6%), cough in 11 patients (9%), restlessness in 6 patients (4.9%), seizures in 8 patients (6.6%), lethargy in 23 patients (18.9%) and not breastfeeding and anorexia in 10 patients (8.2%) were the main complaints. In the age group under 2 months, fever was the most common reason for hospitalization in 68.4%, followed by non-breastfeeding in 36.8%, restlessness and lethargy in 21.1% of patients, and vomiting and seizures in 5.3% of patients. Has been the most common reason for hospitalization. Vomiting, nausea in 47 patients (68.1%), headache in 26 patients (37.7%), nausea in 15 patients (21.7%)
Indifference and cough were the most common causes in 10 patients (14.5%). In the age group over 7 years, the most common reasons for hospitalization were as follows: fever 9 (85.3%), nausea and vomiting 28 (82.4%), headache 26 (76.5%), lethargy 4 People (11.8%), Seizures were observed in 2 patients (5.9%) and cough in 1 patient (2.9%). In the study of blood glucose, the mean hospital stay time in the under 2 months group was 93.42. (Standard deviation 58.67) with a minimum of 29 and a maximum of 251. In the age group of 2 months to the end of 7 years, the mean blood sugar at the time of admission (39.36) was 11.25 with a minimum of 46 and a maximum of 217.
In the age group over 7 years, the mean blood glucose at the time of admission (43.71) was 122.68, with a minimum of 78 and a maximum of 256. In total, only 2 people had hypoglycemia in the age group under 2 months. Of the total number of children, 45 (36.8%) had leukocytosis, of which 2 (16.7%) in the age group under 2 months, 28 (40.6%) in the age group of 2 months to 7 years, and 15 people (44.1%) were in the age group over 7 years. The mean levels of BUN and Cr in the group of children under 2 months are 29.78 (14.6) and 1.24 (2.2), respectively, while in the age group of 2 months to 7 years, these values are respectively (9.9). 17) 25.98 and (65%) 0.66 and in the age group over 7 years are 27.35 (9.4) and 0.64 (17%), respectively.
In the total population of children studied, an increase in BUN in 57 cases (46.7%) was identified, of which 12 (66.7%) in the age group under 2 months, 28 (53.8%) in the age group 2 months to 7 years old and 17 people (65.4%) were in the group of children over 7 years old. Cr level increased in 28 children (22.9%) of which 15 (83.3%) were under 2 months old, 8 (16%) were 2 months to 7 years old and 5 (20%) They are in the age group over 7 years. In the study of electrolytes, the mean level of Na+ in the age group up to 2 months (4.7) was 139.38, in the age group 2 months to 7 years (5.4) 133.61, and in the age group over 7 years (6) 134.81 Was. There were 47 cases (38.5%) in the total population of Hyponatremia, of which 4 cases (3.8%) in the age group under 2 months, 30 cases (58.8%) in the age group 2 months to 7 years, and 13 cases (50%) were over 7 years old in the age group. The mean level of K+ in the age group up to 2 months (84%) was 5.13, in the age group 2 months to 7 years (88%) was 4.13 and in the age group over 7 years (51%) was 3.85. There were 16 cases of hypokalemia, of which 10 patients (19.6%) were in the age group of 2 months to 7 years and 6 patients (235.1) were in the age group over 7 years. In the study of blood culture test results, 188 cases were reported to be negative (96.7%) and 4 cases (3.27%) were reported as positive, including one case of Citrobacter, one case of Pneumococcus, one case of Sod and Mona, and one case of Staphylococcus.
Discussion
Based on the data, we conclude that bacterial meningitis is more common in boys than girls and is most common between the ages of 2 months and 7 years. In the paper, it is mentioned that purulent meningitis is more common in boys than girls. It is most common between the ages of 2 months and 2 years. In the clinical picture, fever was the most common reason for referral. After fever, nausea, restlessness, and lethargy were the most common symptoms in the age group under 2 months, and nausea, vomiting, and headache after fever were the most common symptoms in the two age groups. These results are consistent with the sources mentioned in irritants, restlessness, and non-breastfeeding are significant in young infants and there is usually fever. Older children may experience disturbances of consciousness and back pain, and usually have Corning and Brodsky symptoms if they are diagnosed with bacterial meningitis. Seizures and coma may occur. Elsewhere, acute central nervous system infection is the most common cause of fever along with signs and symptoms of central nervous system disease in children. There were extensive changes in the blood glucose at the time of referral, but the mean blood sugar in all three groups was in the normal range and only two patients had hypoglycemia, which was in the age group of fewer than 2 months, which was probably due to not breastfeeding. The presence of leukocytosis in the age group under 2 months was not a suitable indicator for the diagnosis of bacterial meningitis, while in the two age groups over 2 months, about half of the patients had clear leukocytosis [38].
It is noteworthy that in 101 patients (82.7%) the number of neutrophils constitutes 50% of the number of WBCs, of which 17 (89.7%) in the age group under 2 months, 58 (84%) in the group 2 months to 7 years old and 26 people (76.4%) are in the age group over 7 years. References in the diagnosis of bacterial meningitis do not mention WBC in the blood because the main criterion for diagnosis is based on CSF fluid analysis. The mean levels of BUN and Cr in the age group under 2 months were in the range higher than normal, but in the other two age groups, the mean levels of BUN and Cr were in the acceptable range. In this case, no similar study was performed.
Hyponatremia and hypokalemia are relatively common in the age group above 2 months, while in the age group under 2 months these electrolytes were in the normal range. Hypokalemia is not mentioned in the literature, but Hyponatremia is considered very important due to the syndrome of disproportionate secretion of antidiuretic hormone (SIADH), which causes excessive fluid retention and increases the risk of intracranial pressure. The amount of fluid therapy plays an important role. The incidence of this syndrome has been determined in 30-50% of patients.
The value of blood culture was very weak in confirming the diagnosis of meningitis because no information was recorded for 64 cases (52.4%) and on the other hand in other cases (44.2%) 54 cases were negative and only (3.27%) positive cases have been mentioned. According to blood culture sources, it is positive in 50-90% of patients.
In the study of CSF leukocytes, we concluded that this variable has a high diagnostic value, and this value increases with age, so that in the age group over 7 years, 100% of leukocytes have increased, and in the same study, this We found that in 87.7% of cases neutrophils constitute more than 50% of CSF leukocytes. However, in 2.4% of cases, we did not have information about the percentage of CSF neutrophils. In the remaining 9.9% of cases, they were either TB meningitis or had a positive culture and smear, or the diagnosis was based solely on response to treatment.
Sources also state that in acute bacterial meningitis the number of WBCs in CSF is 60000-100 and elsewhere it is 1000-100 that PMNs often form. In poorly treated bacterial meningitis, the number is 1-1000, and elsewhere is 5-10000, where PMNs are usually predominant, but if the treatment is prolonged, mononuclear cells are predominant. In Tuberculous meningitis, there are 10-500, which are mostly Polymorphonuclear and then mostly lymphocytes and monocytes.
Conclusion
Bacterial meningitis is more common in boys than girls and is more common in the age group of 2 months to 7 years than in other ages. The most common cause is fever.
Acknowledgements: None declared by the authors.
Ethical Permission: None declared by the authors.
Conflicts of Interests: None declared by the authors.
Funding/Support: None declared by the authors.
References
1. Amini A, Shahpoori Arani H, Fard MM. Medical tourism industry: A systematic review on its principles, sequels, and ethical issues. Eurasian J Sci Tech. 2021;2(2):421-4. [Persian] [Link]
2. Fard AM, Fard MM. Evaluation of Office Stones in Kidney Patients and How to form and Treat Them. Eurasian J Sci Tech. 2021;2(2):384-98. [Persian] [Link]
3. Samimi A. New method of corrosion in isomerization units. Advanced J Chem. 2021;4(3):206-18. [Link]
4. Samimi A. Investigation of corrosion metal in oil industry in Iran. Int Innovation Appl Stud. 2012;1(1):1-6. [Link]
5. Samimi A. Investigation of emplacement to impact polyethylene pipes on soil. Int Sci Investigation J. 2014;3(1):57-64. [Link]
6. Samimi A. The need for risk assessment in occupational health. J Eng Ind Res. 2021;2(2):71-6. [Link]
7. Samimi A. Risk management in the laboratory based on the 17025 standards. J Exp Stu Law Manag. 2020;7(3):132-7. [Link]
8. Samimi A. New method of corrosion in isomerization units. Adv J. 2021;4:206-18. [Link]
9. Samimi A. The need for risk assessment in occupational health. J Eng Ind Res. 2021;2:71-6. [Link]
10. Susanabadi A, Sadri MS, Taleby H, Etemadi S, Mahmoodiyeh B, Fard MM. Evaluatingthe outcome of total intravenous anesthesia and single drug pharmacological to prevent postoperative vomiting: systematic review and meta-analysis. Ann Romanian Soc Cell Biol. 2021;25(6):2703-16. [Link]
11. Susanabadi A, Etemadi S, Sadri MS, Mahmoodiyeh B, Taleby H, Fard MM. Comparing transversus abdominis plane block and wound infiltration without liposome anesthetics in adult patients: systematic review and meta-analysis. Ann Romanian Soc Cell Biol. 2021;25(6):2875-87. [Link]
12. Yarahmadi A, Kamrava K, Shafee A, Fard MM, Aghajanpour M, Mohebbi A. Investigation of olfactory function following septorhinoplasty in iranian population by rapid smell test (RST). J Pharm Res Int. 2019;31(6):1-6. [Link] [DOI:10.9734/jpri/2019/v31i630369]
13. 5- Bozorgian A, Zarinabadi S, Samimi A. Optimization of Well Production by Designing a Core pipe in one of the Southwest oil Wells of Iran. J Chem Rev. 2020;2(2):122-9. [Persian] [Link] [DOI:10.33945/SAMI/JCR.2020.2.5]
14. Fard AM, Fard MM. Modeling drug release. Eurasian J Sci Tech. 2021;1(1):284-301. [Persian] [Link]
15. Fard AM, Fard MM. Evaluation of Office Stones in Kidney Patients and How to form and Treat Them. Eurasian J Sci Tech. 2021;2(2):384-98. [Persian] [Link]
16. Shirazi AO, Jahandideh H, Yarahmadi A, Fard MM, Delarestaghi MM. The effect of apple cider vinegar in the treatment of chronic rhinosinusitis. Med Sci. 2020;24(104):2467-74. [Link]
17. Mahmoodiyeh B, Etemadi S, Kamali A, Rajabi S, Fard MM. Evaluating the effect of different types of anesthesia on intraoperative blood glucose levels in diabetics and non-Diabetics Patients: A systematic review and meta-analysis. Ann Romanian Soc Cell Biol. 2021;24(4):2559-72. [Link]
18. Barmasi B. The effect of adding saccharin to the bath on the hardness and wear behavior of the coating. J Eng Ind Res. 2020;1(2):161-9. [Link]
19. Mahdiraji EA, Amiri MS. Optimization of market clearing process in power system with NSGA algorithm. J Eng Ind Res. 2020;1(2):111-22. [Link]
20. Sadr EF, Abadi Z, Sadr NE, Fard M. The risk for SARS-Cov-2 Virus contamination through surgical smoking and aerosolization by laparoscopic surgery: A systematic review . Ann Romanian Soc Cell Biol. 2021;25(1):6839-52. [Link]
21. Gharekhani Kasa F. A study of the architectural design of contemporary museums in Iran. J Eng Ind Res. 2020;1(1);51-74. [Link]
22. Rebout F. CFA performance evaluation: A comprehensive structural equation modeling. J Eng Ind Res. 2020;1(1):19-37. [Link]
23. Zare Kazemabadi F, Heydarinasab A, Akbarzadeh A, Ardjmand M. Preparation, characterization and in vitro evaluation of PEGylated nanoliposomal containing etoposide on lung cancer. Artif Cells Nanomed Biotechnol. 2019;47(1):3222-30. [Link] [DOI:10.1080/21691401.2019.1646265]
24. Zare Kazemabadi F, Heydarinasab A, Akbarzadehkhiyavi A, Ardjmand M. Development, Optimization and In vitro Evaluation of Etoposide loaded Lipid Polymer Hybrid Nanoparticles for controlled Drug Delivery on Lung Cancer. Int J New Chem. 2021;5(2):135-52. [Link]
25. Heydari GH, Hadavand F, Maneshi M, Moatamed N, Vahdat K, Fattah M, et al. Evaluation of resistancy to imipenem in positive blood culture in bushehr educational hospitals -1389. Iran South Med J. 2014;16(6):479-85. [Persian] [Link]
26. Jahandideh H, Yarahmadi A, Rajaieh S, Ostvar Shirazi A, Milanifard M, Yarahmadi A. Cone-beam computed tomography guidance in functional endoscopic sinus surgery: a retrospective cohort study. J Pharm Res Int. 2019;3(6):1-7. [Link] [DOI:10.9734/jpri/2019/v31i630380]
27. Danesh HA. The effect of interventional education on knowledge about medical documentation and medical ethics in the residents of Arak university of medical sciences. Focus Med Sci J. 2018;4:9-13. [Persian] [Link]
28. Danesh HA, Saboury M, Sabzi A, Saboury M, Jafary M, Saboury S. Do not underestimate fournier's gangrene: Report of 8 cases in 10 month survey. Med J Islam Repub Iran. 2015;29(1):105-9. [Persian] [Link]
29. Danesh HA, Javanbakht S, Nourallahzadeh M, Bakhshani NM, Danesh S, Nourallahzadeh F, et al. Epidemiology and mortality of burn injuries in eastern iran since 2009: an analysis of 2115 cases. Int J High Risk Behav Addict. 2019;8(1):e66232. [Persian] [Link] [DOI:10.5812/ijhrba.66232]
30. Otaghvar HR, Afsordeh K, Hosseini M, Mazhari N, Dousti M. Causes of wound dehiscence in trauma patients with penetrating and non-penetrating abdominal wound in Rasool Akram Hospital within 2017-2020. J Surg Trauma. 2020;8(4):156-60. [Persian] [Link] [DOI:10.32592/jsurgery.2020.8.4.105]
31. Otaghvar HR, Baniahmad M, Pashazadeh AM, Nabipour I, Javadi H, Rezaei L, et al. The role of 99mTc-Ubiquicidin (UBI) and 99mTc-IgG scintigraphies in diagnosis of acute appendicitis: A preliminary result. Iran J Nucl Med. 2014;22(1):7-10. [Link]
32. Otaghvar HR, Hoseini M, Mirmalek A, Ahmari H, Arab F, Amiri Mohtasham N. BREAST sarcoma: A review article. Iran J Surg. 2014;22(1):1-11. [Link]
33. Otaghvar HR, Soleymanzadeh P, Hosseini H, Karbalaei-Esmaeili S. Primary breast angiosarcoma associated with abnormalities in international normalized ratio platelet count and anemia. J Cancer Res Ther. 2015;11(3):655. [Link] [DOI:10.4103/0973-1482.139346]
34. Otaghvar HR, Firoozbakht S, Montazeri S, Khazraie S, Bani Ahmad M, Hajiloo M. A remarkable improvement of patients with idiopathic thrombocytopenic purpura after appendectomy including carcinoid tumor. ISMJ. 2011;14(2):134-9. [Link]
35. Zeidi IM, Morshedi H, Otaghvar HR. A theory of planned behavior-enhanced intervention to promote health literacy and self-care behaviors of type 2 diabetic patients. JPMH. 2020;61(4):E601-13. [Link]
36. Ghajarzadeh K, Fard MM, Alizadeh Otaghvar H, Faiz SH, Dabbagh A, Mohseni M, et al. The effect of educational curriculum implementation related to tracheal intubation on preventing clinical and psychological consequences of COVID-19 among intensive care unit personnel. Ann Romanian Soc Cell Biol. 2021;25(2):2449-56. [Link]
37. Ghajarzadeh K, Fard MM, Alizadeh Otaghvar H, Faiz SH, Dabbagh A, Mohseni M, et al. Effects of dexmedetomidine and propofol on hemodynamic stability and ventilation time in patients suffering COVID-19 admitting to intensive care units. Ann Romanian Soc Cell Biol. 2021;25(2):2457-65. [Link]
38. Ghajarzadeh.K, MilaniFard.M, Alebouyeh MR, Alizadeh Otaghvar H, Dabbagh A, Mohseni M, et al. The prominent chest CT findings in Covid-19 patients: A systematic review and meta-analysis. Ann Romanian Soc Cell Biol. 2021;25(2):2466-84. [Link]