GMJ Medicine
eISSN : 2626-3041

Embase

Biosis Previews
description
Volume 3, Issue 1 (2024)
GMJM 2024, 3(1): 31-36 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2023/08/8 | Accepted: 2024/01/4 | Published: 2024/02/15
Received: 2023/08/8 | Accepted: 2024/01/4 | Published: 2024/02/15
How to cite this article
Shiravand M, Safikhani H. Effect of Open- Versus Closed Exercises on Psychological Function in Children with Tic Disorder. GMJM 2024; 3 (1) :31-36
URL: http://gmedicine.de/article-2-220-en.html
URL: http://gmedicine.de/article-2-220-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

Authors
M. Shiravand *1, H. Safikhani1
1- Department of Physical Education, Kermanshah Branch, Islamic Azad University, Kermanshah, Iran
Keywords:
| Abstract (HTML) (1493 Views)
Full-Text: (396 Views)
Introduction
Tourette syndrome (TS) is a neurodevelopmental disorder that is known by the presence of motor and vocal tics for at least 1 year [1]. Tics are commonly transient disorders in childhood and are considered a normal part of development, but some children show persistence [2]. Motor tics are often sudden, short, and meaningless. Some motor tics include blinking, grimacing, and head, nose twitching, mouth and shoulder movements. Tics often influence psychosocial functioning in children and their families [2]. Most children referred to clinics for treatment of motor tic have neuropsychiatric conditions such as attention deficit hyperactivity disorder and obsessive-compulsive [3]. Psychiatric diagnoses usually show anxiety disorders by 85% in childhood [3]. Parents and children usually report distressed behaviors related to faults in daily functioning and anxiety disorders [4]. Different interventions are used for the alleviation of psychological symptoms in patients with tic syndrome. Drug interventions usually have side effects and are not efficient for all patients [2]. Physical activities have been interesting due to their beneficial effects on health. Exercises are commonly used for the prevention and management of chronic diseases [5].
The beneficial effects of regular physical activity on health are indisputable in the field of modern medicine. Exercise is often the first step in lifestyle modification for the prevention and management of chronic diseases. Regular exercise creates physiological changes and adaptations in the human body by influencing hypothalamic pituitary–adrenal (HPA) axis reactivity [6, 7]. This axis plays an important role in extending adaptive responses to physical and psychological stressors [8]. Faults in the HPA cause depressive and anxiety signs [9].
Open- and closed-skill exercises have been interesting. Open-skill exercises are known as skills that players need to react in a dynamically changing, unpredictable, and externally paced environment, such as basketball, tennis, fencing, etc. [10]. Closed-skill exercises, known as exercises in that sporting environment, are relatively consistent, predictable, and self-paced for players, such as running and swimming [10]. Athletes from open-skill sports may develop more flexibility in visual attention, decision-making, and action execution versus athletes from closed-skill sports [11]. Studies have reported the effects of open- and closed-skill exercise on neuropsychological actions in disabled athletes and young adults and also neurocognitive functions in the elderly [12, 13]. Studies have reported that subjects who participated in open-skill exercises showed better neurocognitive performances versus those who participated in closed skills [14, 15]. It seems that open- and closed-skill exercises could improve psychological function in children with motor tics. Psychological disorders are part of tic syndrome that has received little attention from the scientific community. In addition, to the best of our knowledge, no study has been conducted to evaluate the effect of open- versus closed-skill exercises on psychological function in children with tic disorder. This study was thus conducted to evaluate the effect of open- versus closed-skill exercises on psychological function in children with tic disorder. The main hypothesis was that open exercises have better efficiency in psychological performance compared to closed exercises.
Materials and Methods
Participants
Sixty boy children ranging from 10 to 12 years of age (11.12±0.83) participated in the experiment and completed evaluations at post-test. Body weight (in shorts and t-shirt) and height (without shoes) were investigated by an electronic scale and converted to body mass index or BMI. Children were randomly selected from local elementary schools in the Kermanshah Province, West region. The inclusion criteria were as follows: (1) Consent of children for participation in the study, (2) children aged between 10 and 12 years of age, (3) children had no medical condition that would affect study results or limit physical activity, (4) children with tic severity >2 and (5) children were not taking medication that would affect study results (e.g. antipsychotics). Exclusion criteria included: (1) Children did not have tendency for participation in this study, (2) children with tic severity <2, (3) consumption of drugs that would affect study results or limit physical activity, (4) the use of antipsychotics and (5) non-participating in exercises for at least two meetings (Figure 1).
Study procedure
This randomized controlled trial was carried out for 8 weeks in children’s with motor tics. Sixty boy children were randomly assigned into three groups including: (1) Closed treatment that children exercised closed exercises for 45 min per session, (2) open treatment that children exercised open exercises for 45 min per session, and (3) who did not have any exercise or control condition. Consents were provided from parents all the subjects before participating their children. Children and their parents completed written informed consent. Children assigned to exercise treatments attended programs that met 3 days per week for 8 weeks.
Yale Global Tic Severity Scale
The Yale global tic severity scale is a clinician-rated measure of tic severity over the last 7-10 days. It has a stable factor structure and excellent psychometric properties. The motor and tics are rated on a 0-5 scale across five dimensions: number, frequency, intensity, complexity, and interference.
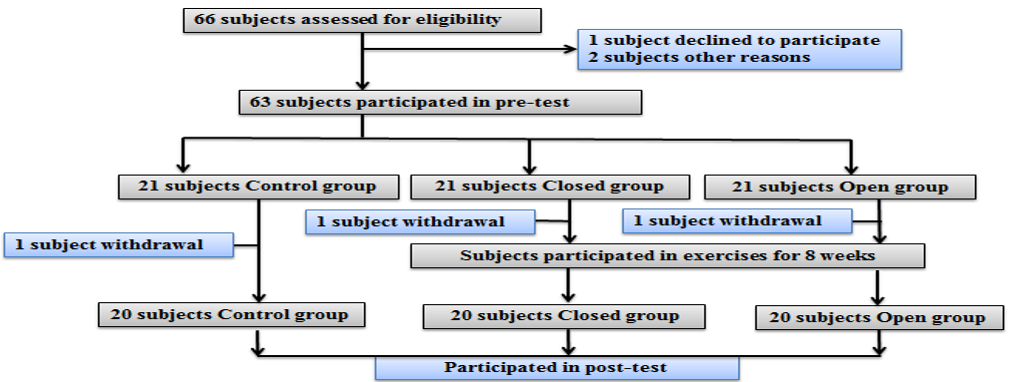
Figure 1. Flowchart of the study
Exercise intervention
The exercise sessions were carried out after school during consecutive sessions. Children were transported by bus to a training place in Kermanshah City. Instructors included master’s level physical educators, bachelor’s level exercise scientists, and other trained research staff who had at least some college education. In this study, we emphasized enjoyment and safety but no competition. Intervention modulations in the open group included 5 min daily warm-up (brisk walking and jumping jacks) and 40 min tennis exercise by instructors. Intervention modulations in the closed group included 5 min daily warm-up (brisk walking and jumping jacks) and 40 min running on a treadmill. Parents completed Spence Children’s Anxiety Scale Child and Parent Versions (SCAS-C; Spence, 1998) in pre-test (pre-interventions) and post-test (after 8-week exercises). The questionnaire included 38 items rated on a 4-point scale (0 to 3; never to always), and the SCAS-C includes six additional positive filler items. The SCAS-C/P comprises six subscales addressing Separation Anxiety (six items), Generalized Anxiety (six items), Social Phobia (six items), Obsessive–Compulsive Behaviors (six items), Panic and Agoraphobia (nine items), and Physical Injury Fears (five items).
Statistical analysis
This study was carried out in a 2×3 factorial arrangement with the effect of time (pre-test & post-test) and exercises (Control, Closed & Open) and their interaction. The data were reported as mean±SD. The data were analyzed for the main effects of time and exercise and the interactions between time and exercise. Where the interaction effect was significant, the effects of the main factors were not considered. The data were analyzed by using SPSS 23 software. Comparisons between groups were conducted by Scheffe test and paired-tests were conducted by T-test. Kolmogorov-Smirnov test was used to test the normality.
Findings
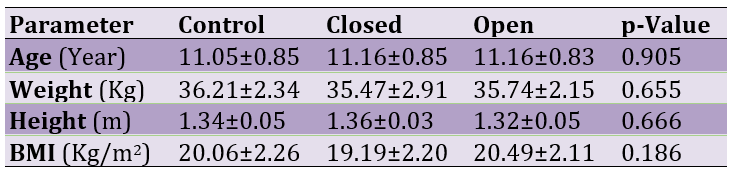
The results showed that the mean age, weight, height, and BMI were 11.12±0.83, 35.81±2.47, 1.34±0.05, and 19.91±2.22, respectively. There were no significant differences between groups (p>0.05; Table 1).
Table 1. Comparing the mean of subjects’ characteristics
Yale Global Tic Severity scale
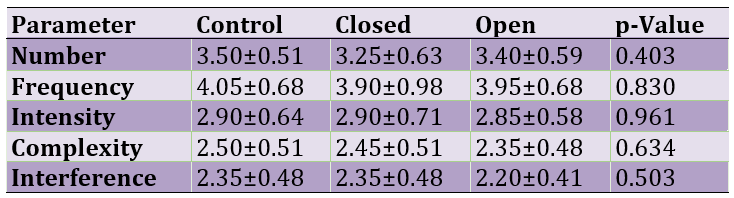
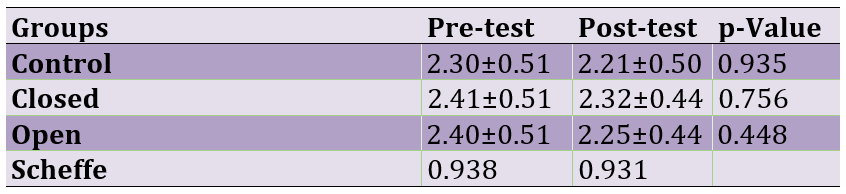
Values for number, frequency, intensity, complexity, and interference were 3.38±0.58, 3.96±0.78, 2.88±0.64, 2.43±0.49, and 2.30±0.46, respectively. There were no significant differences between groups (p>0.05; Table 2).
Table 2. Distribution of Yale Global Tic Severity scale scores across participants (Mean±SD)
The effect of skill exercises on Separation Anxiety
The effect of open- and closed-skill exercises on Separation Anxiety is shown in Table 4. The results for the effect of open- and closed-skill exercises on Separation Anxiety were as follows: For the effect of time [F(1, 59)=7.10; p=0.0009], exercise [F(2, 59)=1.41; p=0.247] and time×exercise interaction [F(1, 59)=4.38; p=0.015]. Scheffe test showed a significant difference between groups in the post-test (p=0.006). The results showed that open exercise, but no closed test decreased Separation Anxiety (Figure 2).
Table 4. Comparing the mean of skill exercises on separation anxiety in pre- and post-test

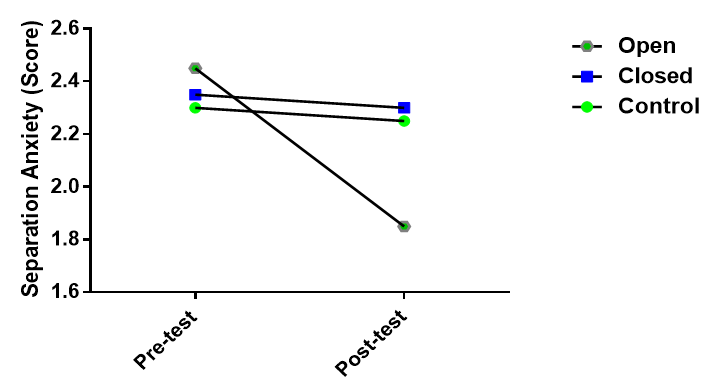
Figure 2. Effect of skill exercises on Separation Anxiety in pre- and Post-test
The effect of skill exercises on Panic and Agoraphobia
The results for the effect of open- and closed-skill exercises on Panic and Agoraphobia are presented in Table 5. The results for the effect of open- and closed-skill exercises on Panic and Agoraphobia were including: The effect of time [F(1, 59)=7.08; p=0.0009], exercise [F(2, 59)=4.22; p=0.017] and time×exercise interaction [F(1, 59)=5.67; p=0.004]. There was a significant response for the Scheffe test in the post-test (p=0.008). The results showed that open exercise but no closed test decreased Panic and Agoraphobia (Figure 3), so the scores were 2.40±0.50 and 1.75±0.44 in the pre-and post-test, respectively.
Table 5. Effect of Skill Exercises on Panic and Agoraphobia in Pre- and post-test
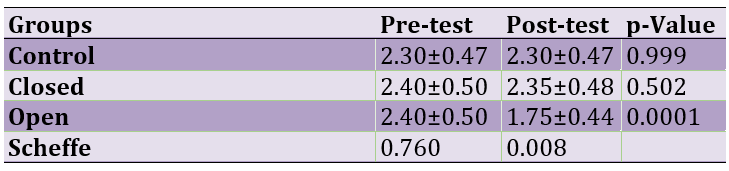
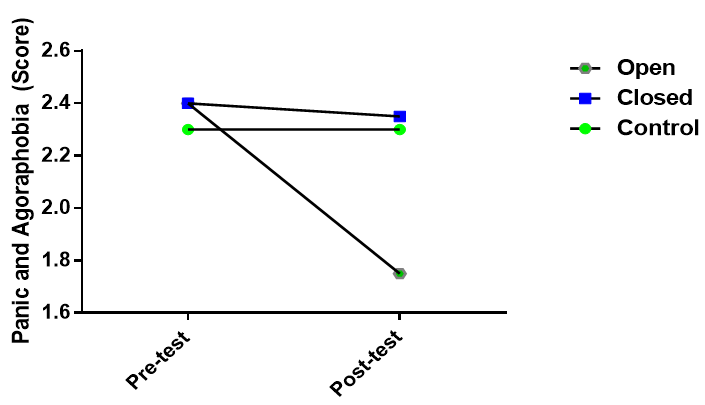
Figure 3. Effect of Skill Exercises on Panic and Agoraphobia in pre- and Post-test
The effect of skill exercises on Physical Injury Fears
Table 6 shows the effect of open and closed-skill exercises on Physical Injury Fears. The results for the effect of open- and closed-skill exercises on Physical Injury Fears were as follows: For the effect of time [F(1, 59)=31.48; p=0.000], exercise [F(2, 59)=5.48; p=0.005] and time×exercise interaction [F(1, 59)= 6.39; p=0.002]. Scheffe test showed a significant difference between groups in the post-test (p=0.0001). The results showed that open and closed-skill exercises decreased Physical Injury Fears (Figure 4).
Table 6. Effect of Skill Exercises on Physical Injury Fears in Pre- and post-test
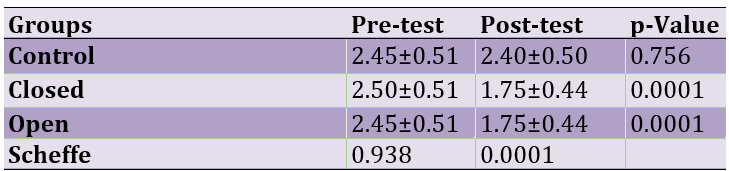
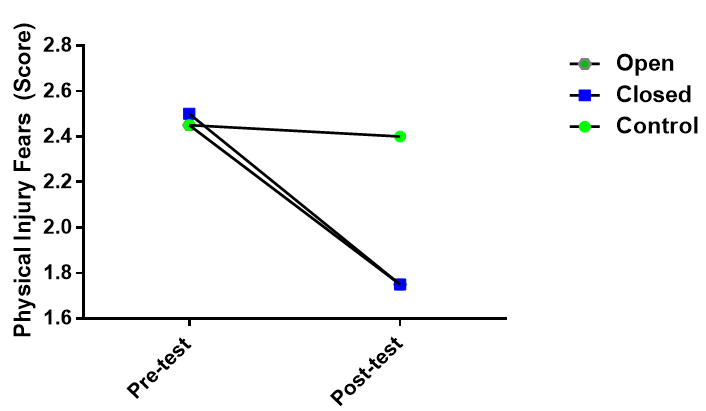
Figure 4. Effect of skill exercises on physical injury fears in pre- and post-test
The effect of exercises on Generalized Anxiety
The results for the effect of open- and closed-skill exercises on Generalized Anxiety are presented in Table 7. The results for the effect of open- and closed-skill exercises on Generalized Anxiety included: The effect of time [F(1, 59)=4.20, p=0.043], exercise [F(2, 59)=2.18, p=0.117] and time×exercise interaction [F(1, 59)=1.49, p=0.229]. There was a significant response for the Scheffe test in the post-test (p=0.0244). The results showed that open exercise but no closed test decreased Generalized Anxiety (Figure 5), so the score was 2.45±0.51 and 2.05±0.39 in the pre-and post-test, respectively.
Table 7. Effect of Skill Exercises on Generalized Anxiety in Pre- and post-test
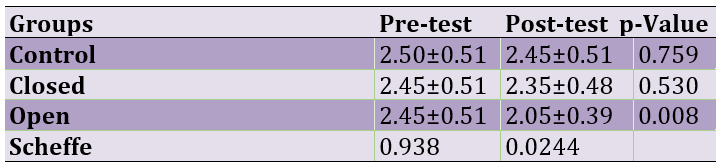
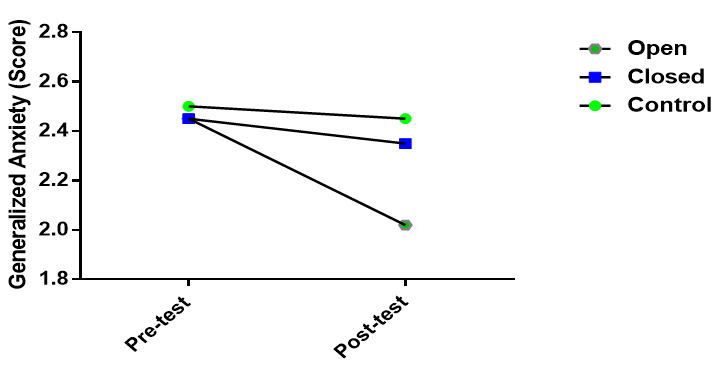
Figure 5. Effect of skill exercises on generalized anxiety in pre- and post-test
The effect of exercises on Social Phobia and Obsessive–Compulsive
The results for the effects of open- and closed-skill exercises on Social Phobia and Obsessive-Compulsive are shown in Tables 8 and 9. The results for the effect of open- and closed-skill exercises on Social Phobia included: The effect of time [F (1, 59)=0.48; p=0.856], exercise [F(2, 59)=0.51; p=0.812] and time×exercise interaction [F(1, 59)=0.39; p=0.962]. The results also for the effect of open- and closed-skill exercises on obsessive-compulsive were as follows: The effect of time [F(1, 59)=0.35; p=0.756], exercise [F(2, 59)=0.21; p=0.812] and time×exercise interaction [F(1, 59)=0.46; p=0.662]. There was no significant difference between groups for the effects of closed- and open-skill exercises on Social Phobia and Obsessive-Compulsive (p>0.05).
Table 8. Effect of skill exercises on social phobia in pre- and post-test
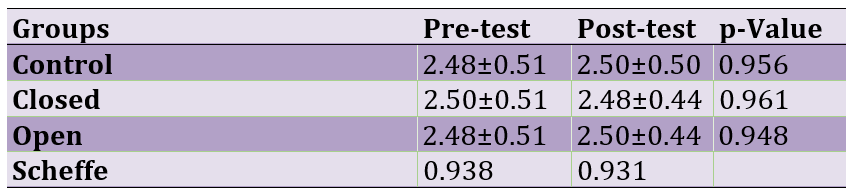
Table 9. Effect of skill exercises on obsessive-compulsive in pre- and post-test
Discussion
Our findings provided evidence for the effects of open exercises on some psychological parameters versus closed exercises. Empirical support for the hypothesis that open-skill exercise has a positive effect on alleviation of Separation Anxiety, Panic and Agoraphobia, Physical Injury Fears, and Generalized Anxiety. Unfortunately, we could not find any study to show the effects of open- and closed exercises on psychological parameters in children with motor tics. In contrast to our findings, Strohle et al. [16] evaluated the effects of quiet rest or aerobic treadmill exercise on anti-panic and anxiolytic activity in patients with panic disorder and showed that anxiety was significantly higher in patients submitted to treadmill exercise. The difference between our findings and Strohle et al. could be attributed to physiological conditions in subjects because people with panic disorder have higher anxiety. Another study showed that patients with panic disorder who participated in aerobic exercise, including walking or running, showed lower anxiety symptoms [17]. It was reported that physical activity influences attention, depression, anxiety, and overall well-being [18]. It was reported that physical exercises increase cardiorespiratory fitness, which is related to improvements in the neuropsychological and electrophysiological performance of working memory in pre-adolescent children [19].
Animal studies have reported that physical activity decreases anxiety-like behavior in rodents. One study evaluated the effects of long-term wheel running on anxiety-like behavior in transgenic mice and reported a reduction [20].
Other studies have reported positive effects of physical activity on depression, cognition, hippocampus changes, and cognitive impairments in neurodegenerative diseases [21].
Physical activity increases neurogenesis in animal hippocampus and new neurons and reduces anxiety-like behavior or hippocampal activation. Studies have not reported the effects of closed- and open-skill exercises on anxiety and other psychological performances. However, previous studies have reported that regular participation in open- and closed-skill exercise has beneficial effects on neurocognitive performances (e.g., specific cost, RT, P3 amplitudes, and strength of inhibitory control) in the elderly when performing the task-switching paradigm [12] and visuospatial attention task [13]. In this study, open-skill exercises could significantly decrease fear and anxiety compared to closed-skill exercises. The difference between exercises could be attributed to the type of exercise and where exercises influence the brain. Previous studies have reported that open-skill exercise (e.g., table tennis) influences more of the prefrontal cortex which is responsible for attention, task-switching, and inhibition, but closed-skill exercise (e.g., jogging) affects more on the hippocampus, which is responsible for memory [22].
In this study, we tried to minimize a number of confounding factors that could mediate the exercise–psychological variables association, but some potential limitations of this work need to be investigated. The results of this study should not be generalized to all children with tic syndrome. In this study, we only investigated motor tics. There is a need to conduct comprehensive studies.
Conclusion
Open-skill exercises decrease some psychological parameters in children with tic syndrome. It can be suggested to use open exercises but not closed exercises to decrease psychological symptoms.
Acknowledgments: None declared by the authors.
Ethical Permissions: A local Ethical Committee (Physical Education Review Board of Islamic Azad University, Kermanshah-Iran approved all procedures used in this study (No permission, IAUKI, 15201).
Conflicts of Interests: None declared by the authors.
Funding/Support: This work was supported by Islamic Azad University, Kermanshah Branch, Kermanshah-Iran.
Tourette syndrome (TS) is a neurodevelopmental disorder that is known by the presence of motor and vocal tics for at least 1 year [1]. Tics are commonly transient disorders in childhood and are considered a normal part of development, but some children show persistence [2]. Motor tics are often sudden, short, and meaningless. Some motor tics include blinking, grimacing, and head, nose twitching, mouth and shoulder movements. Tics often influence psychosocial functioning in children and their families [2]. Most children referred to clinics for treatment of motor tic have neuropsychiatric conditions such as attention deficit hyperactivity disorder and obsessive-compulsive [3]. Psychiatric diagnoses usually show anxiety disorders by 85% in childhood [3]. Parents and children usually report distressed behaviors related to faults in daily functioning and anxiety disorders [4]. Different interventions are used for the alleviation of psychological symptoms in patients with tic syndrome. Drug interventions usually have side effects and are not efficient for all patients [2]. Physical activities have been interesting due to their beneficial effects on health. Exercises are commonly used for the prevention and management of chronic diseases [5].
The beneficial effects of regular physical activity on health are indisputable in the field of modern medicine. Exercise is often the first step in lifestyle modification for the prevention and management of chronic diseases. Regular exercise creates physiological changes and adaptations in the human body by influencing hypothalamic pituitary–adrenal (HPA) axis reactivity [6, 7]. This axis plays an important role in extending adaptive responses to physical and psychological stressors [8]. Faults in the HPA cause depressive and anxiety signs [9].
Open- and closed-skill exercises have been interesting. Open-skill exercises are known as skills that players need to react in a dynamically changing, unpredictable, and externally paced environment, such as basketball, tennis, fencing, etc. [10]. Closed-skill exercises, known as exercises in that sporting environment, are relatively consistent, predictable, and self-paced for players, such as running and swimming [10]. Athletes from open-skill sports may develop more flexibility in visual attention, decision-making, and action execution versus athletes from closed-skill sports [11]. Studies have reported the effects of open- and closed-skill exercise on neuropsychological actions in disabled athletes and young adults and also neurocognitive functions in the elderly [12, 13]. Studies have reported that subjects who participated in open-skill exercises showed better neurocognitive performances versus those who participated in closed skills [14, 15]. It seems that open- and closed-skill exercises could improve psychological function in children with motor tics. Psychological disorders are part of tic syndrome that has received little attention from the scientific community. In addition, to the best of our knowledge, no study has been conducted to evaluate the effect of open- versus closed-skill exercises on psychological function in children with tic disorder. This study was thus conducted to evaluate the effect of open- versus closed-skill exercises on psychological function in children with tic disorder. The main hypothesis was that open exercises have better efficiency in psychological performance compared to closed exercises.
Materials and Methods
Participants
Sixty boy children ranging from 10 to 12 years of age (11.12±0.83) participated in the experiment and completed evaluations at post-test. Body weight (in shorts and t-shirt) and height (without shoes) were investigated by an electronic scale and converted to body mass index or BMI. Children were randomly selected from local elementary schools in the Kermanshah Province, West region. The inclusion criteria were as follows: (1) Consent of children for participation in the study, (2) children aged between 10 and 12 years of age, (3) children had no medical condition that would affect study results or limit physical activity, (4) children with tic severity >2 and (5) children were not taking medication that would affect study results (e.g. antipsychotics). Exclusion criteria included: (1) Children did not have tendency for participation in this study, (2) children with tic severity <2, (3) consumption of drugs that would affect study results or limit physical activity, (4) the use of antipsychotics and (5) non-participating in exercises for at least two meetings (Figure 1).
Study procedure
This randomized controlled trial was carried out for 8 weeks in children’s with motor tics. Sixty boy children were randomly assigned into three groups including: (1) Closed treatment that children exercised closed exercises for 45 min per session, (2) open treatment that children exercised open exercises for 45 min per session, and (3) who did not have any exercise or control condition. Consents were provided from parents all the subjects before participating their children. Children and their parents completed written informed consent. Children assigned to exercise treatments attended programs that met 3 days per week for 8 weeks.
Yale Global Tic Severity Scale
The Yale global tic severity scale is a clinician-rated measure of tic severity over the last 7-10 days. It has a stable factor structure and excellent psychometric properties. The motor and tics are rated on a 0-5 scale across five dimensions: number, frequency, intensity, complexity, and interference.
Figure 1. Flowchart of the study
Exercise intervention
The exercise sessions were carried out after school during consecutive sessions. Children were transported by bus to a training place in Kermanshah City. Instructors included master’s level physical educators, bachelor’s level exercise scientists, and other trained research staff who had at least some college education. In this study, we emphasized enjoyment and safety but no competition. Intervention modulations in the open group included 5 min daily warm-up (brisk walking and jumping jacks) and 40 min tennis exercise by instructors. Intervention modulations in the closed group included 5 min daily warm-up (brisk walking and jumping jacks) and 40 min running on a treadmill. Parents completed Spence Children’s Anxiety Scale Child and Parent Versions (SCAS-C; Spence, 1998) in pre-test (pre-interventions) and post-test (after 8-week exercises). The questionnaire included 38 items rated on a 4-point scale (0 to 3; never to always), and the SCAS-C includes six additional positive filler items. The SCAS-C/P comprises six subscales addressing Separation Anxiety (six items), Generalized Anxiety (six items), Social Phobia (six items), Obsessive–Compulsive Behaviors (six items), Panic and Agoraphobia (nine items), and Physical Injury Fears (five items).
Statistical analysis
This study was carried out in a 2×3 factorial arrangement with the effect of time (pre-test & post-test) and exercises (Control, Closed & Open) and their interaction. The data were reported as mean±SD. The data were analyzed for the main effects of time and exercise and the interactions between time and exercise. Where the interaction effect was significant, the effects of the main factors were not considered. The data were analyzed by using SPSS 23 software. Comparisons between groups were conducted by Scheffe test and paired-tests were conducted by T-test. Kolmogorov-Smirnov test was used to test the normality.
Findings
The results showed that the mean age, weight, height, and BMI were 11.12±0.83, 35.81±2.47, 1.34±0.05, and 19.91±2.22, respectively. There were no significant differences between groups (p>0.05; Table 1).
Table 1. Comparing the mean of subjects’ characteristics
Yale Global Tic Severity scale
Values for number, frequency, intensity, complexity, and interference were 3.38±0.58, 3.96±0.78, 2.88±0.64, 2.43±0.49, and 2.30±0.46, respectively. There were no significant differences between groups (p>0.05; Table 2).
Table 2. Distribution of Yale Global Tic Severity scale scores across participants (Mean±SD)
The effect of skill exercises on Separation Anxiety
The effect of open- and closed-skill exercises on Separation Anxiety is shown in Table 4. The results for the effect of open- and closed-skill exercises on Separation Anxiety were as follows: For the effect of time [F(1, 59)=7.10; p=0.0009], exercise [F(2, 59)=1.41; p=0.247] and time×exercise interaction [F(1, 59)=4.38; p=0.015]. Scheffe test showed a significant difference between groups in the post-test (p=0.006). The results showed that open exercise, but no closed test decreased Separation Anxiety (Figure 2).
Table 4. Comparing the mean of skill exercises on separation anxiety in pre- and post-test
Figure 2. Effect of skill exercises on Separation Anxiety in pre- and Post-test
The effect of skill exercises on Panic and Agoraphobia
The results for the effect of open- and closed-skill exercises on Panic and Agoraphobia are presented in Table 5. The results for the effect of open- and closed-skill exercises on Panic and Agoraphobia were including: The effect of time [F(1, 59)=7.08; p=0.0009], exercise [F(2, 59)=4.22; p=0.017] and time×exercise interaction [F(1, 59)=5.67; p=0.004]. There was a significant response for the Scheffe test in the post-test (p=0.008). The results showed that open exercise but no closed test decreased Panic and Agoraphobia (Figure 3), so the scores were 2.40±0.50 and 1.75±0.44 in the pre-and post-test, respectively.
Table 5. Effect of Skill Exercises on Panic and Agoraphobia in Pre- and post-test
Figure 3. Effect of Skill Exercises on Panic and Agoraphobia in pre- and Post-test
The effect of skill exercises on Physical Injury Fears
Table 6 shows the effect of open and closed-skill exercises on Physical Injury Fears. The results for the effect of open- and closed-skill exercises on Physical Injury Fears were as follows: For the effect of time [F(1, 59)=31.48; p=0.000], exercise [F(2, 59)=5.48; p=0.005] and time×exercise interaction [F(1, 59)= 6.39; p=0.002]. Scheffe test showed a significant difference between groups in the post-test (p=0.0001). The results showed that open and closed-skill exercises decreased Physical Injury Fears (Figure 4).
Table 6. Effect of Skill Exercises on Physical Injury Fears in Pre- and post-test
Figure 4. Effect of skill exercises on physical injury fears in pre- and post-test
The effect of exercises on Generalized Anxiety
The results for the effect of open- and closed-skill exercises on Generalized Anxiety are presented in Table 7. The results for the effect of open- and closed-skill exercises on Generalized Anxiety included: The effect of time [F(1, 59)=4.20, p=0.043], exercise [F(2, 59)=2.18, p=0.117] and time×exercise interaction [F(1, 59)=1.49, p=0.229]. There was a significant response for the Scheffe test in the post-test (p=0.0244). The results showed that open exercise but no closed test decreased Generalized Anxiety (Figure 5), so the score was 2.45±0.51 and 2.05±0.39 in the pre-and post-test, respectively.
Table 7. Effect of Skill Exercises on Generalized Anxiety in Pre- and post-test
Figure 5. Effect of skill exercises on generalized anxiety in pre- and post-test
The effect of exercises on Social Phobia and Obsessive–Compulsive
The results for the effects of open- and closed-skill exercises on Social Phobia and Obsessive-Compulsive are shown in Tables 8 and 9. The results for the effect of open- and closed-skill exercises on Social Phobia included: The effect of time [F (1, 59)=0.48; p=0.856], exercise [F(2, 59)=0.51; p=0.812] and time×exercise interaction [F(1, 59)=0.39; p=0.962]. The results also for the effect of open- and closed-skill exercises on obsessive-compulsive were as follows: The effect of time [F(1, 59)=0.35; p=0.756], exercise [F(2, 59)=0.21; p=0.812] and time×exercise interaction [F(1, 59)=0.46; p=0.662]. There was no significant difference between groups for the effects of closed- and open-skill exercises on Social Phobia and Obsessive-Compulsive (p>0.05).
Table 8. Effect of skill exercises on social phobia in pre- and post-test
Table 9. Effect of skill exercises on obsessive-compulsive in pre- and post-test
Discussion
Our findings provided evidence for the effects of open exercises on some psychological parameters versus closed exercises. Empirical support for the hypothesis that open-skill exercise has a positive effect on alleviation of Separation Anxiety, Panic and Agoraphobia, Physical Injury Fears, and Generalized Anxiety. Unfortunately, we could not find any study to show the effects of open- and closed exercises on psychological parameters in children with motor tics. In contrast to our findings, Strohle et al. [16] evaluated the effects of quiet rest or aerobic treadmill exercise on anti-panic and anxiolytic activity in patients with panic disorder and showed that anxiety was significantly higher in patients submitted to treadmill exercise. The difference between our findings and Strohle et al. could be attributed to physiological conditions in subjects because people with panic disorder have higher anxiety. Another study showed that patients with panic disorder who participated in aerobic exercise, including walking or running, showed lower anxiety symptoms [17]. It was reported that physical activity influences attention, depression, anxiety, and overall well-being [18]. It was reported that physical exercises increase cardiorespiratory fitness, which is related to improvements in the neuropsychological and electrophysiological performance of working memory in pre-adolescent children [19].
Animal studies have reported that physical activity decreases anxiety-like behavior in rodents. One study evaluated the effects of long-term wheel running on anxiety-like behavior in transgenic mice and reported a reduction [20].
Other studies have reported positive effects of physical activity on depression, cognition, hippocampus changes, and cognitive impairments in neurodegenerative diseases [21].
Physical activity increases neurogenesis in animal hippocampus and new neurons and reduces anxiety-like behavior or hippocampal activation. Studies have not reported the effects of closed- and open-skill exercises on anxiety and other psychological performances. However, previous studies have reported that regular participation in open- and closed-skill exercise has beneficial effects on neurocognitive performances (e.g., specific cost, RT, P3 amplitudes, and strength of inhibitory control) in the elderly when performing the task-switching paradigm [12] and visuospatial attention task [13]. In this study, open-skill exercises could significantly decrease fear and anxiety compared to closed-skill exercises. The difference between exercises could be attributed to the type of exercise and where exercises influence the brain. Previous studies have reported that open-skill exercise (e.g., table tennis) influences more of the prefrontal cortex which is responsible for attention, task-switching, and inhibition, but closed-skill exercise (e.g., jogging) affects more on the hippocampus, which is responsible for memory [22].
In this study, we tried to minimize a number of confounding factors that could mediate the exercise–psychological variables association, but some potential limitations of this work need to be investigated. The results of this study should not be generalized to all children with tic syndrome. In this study, we only investigated motor tics. There is a need to conduct comprehensive studies.
Conclusion
Open-skill exercises decrease some psychological parameters in children with tic syndrome. It can be suggested to use open exercises but not closed exercises to decrease psychological symptoms.
Acknowledgments: None declared by the authors.
Ethical Permissions: A local Ethical Committee (Physical Education Review Board of Islamic Azad University, Kermanshah-Iran approved all procedures used in this study (No permission, IAUKI, 15201).
Conflicts of Interests: None declared by the authors.
Funding/Support: This work was supported by Islamic Azad University, Kermanshah Branch, Kermanshah-Iran.
References
1. Nosratmirshekarlou E, Shafiq S, Goodarzi ZS, Martino D, Pringsheim T. Effect of diet, exercise and sleep on tic severity: a scoping review protocol. BMJ Open. 2019;9:e024653. [Link] [DOI:10.1136/bmjopen-2018-024653]
2. Robertson MM, Chowdhury U. Behavioral and psychological therapies for Tourette syndrome and tic disorders: Their place in treatment and history. Neuropsychiatry. 2011;1(4):385-400. [Link] [DOI:10.2217/npy.11.38]
3. Hirschtritt ME, Lee PC, Pauls DL, Dion Y, Grados MA, Illmann C, et al. Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome. JAMA Psychiatry. 2015;72(4):325-33. [Link] [DOI:10.1001/jamapsychiatry.2014.2650]
4. Robinson S, Hindley P, Hedderly T. Tic attacks: panic disorder in Tourette syndrome. Front Pediatr. 2016;4:46. [Link] [DOI:10.3389/fped.2016.00046]
5. Anderson E, Shivakumar G. Effects of exercise and physical activity on anxiety. Front Psychiatry. 2013;4:27. [Link] [DOI:10.3389/fpsyt.2013.00027]
6. Jackson EM, Dishman RK. Cardiorespiratory fitness and laboratory stress: A meta-regression analysis. Psychophysiol. 2006;43(1):57-72. [Link] [DOI:10.1111/j.1469-8986.2006.00373.x]
7. Rimmele U, Zellweger BC, Marti B, Seiler R, Mohiyeddini C, Ehlert U, et al. Trained men show lower cortisol, heart rate and psychological responses to psychosocial stress compared with untrained men. Psychoneuroendocrinol. 2007;32(6):627-35. [Link] [DOI:10.1016/j.psyneuen.2007.04.005]
8. De Kloet ER, Joëls M, Holsboer F. Stress and the brain: From adaptation to disease. Nat Rev Neurosci. 2005;6(6):463-75. [Link] [DOI:10.1038/nrn1683]
9. Landgraf R, Wigger A, Holsboer F, Neumann I. Hyper-reactive hypothalamo-pituitary-adrenocortical axis in rats bred for high anxiety-related behaviour. J Neuroendocrinol. 1999;11(6):405-7. [Link] [DOI:10.1046/j.1365-2826.1999.00342.x]
10. Di Russo F, Bultrini A, Brunelli S, Delussu AS, Polidori L, et al. Benefits of sports participation for executive function in disabled athletes. J Neurotrauma. 2010;27(12):2309-19. [Link] [DOI:10.1089/neu.2010.1501]
11. Taddei F, Bultrini A, Spinelli D, Di Russo F. Neural correlates of attentional and executive processing in middle-aged fencers. Med Sci Sport Exer. 2012;44(6):1057-66. [Link] [DOI:10.1249/MSS.0b013e31824529c2]
12. Tsai CL, Wang WL. Exercise-mode-related changes in task-switching performance in the elderly. Front Behav Neurosci. 2015;9:56. [Link] [DOI:10.3389/fnbeh.2015.00056]
13. Tsai CL, Wang CH, Chen F. Pan CY. Huang SY, Tseng YT. The effects of different exercise types on visuospatial attention in the elderly. Psychol Sport Exer. 2016;26:130-8. [Link] [DOI:10.1016/j.psychsport.2016.06.013]
14. Wang CH, Chang CC, Liang YM, Chiu WS, Tseng P, Hung DL, et al. Open vs. closed sports and the modulation of inhibitory control. PLoS ONE. 2013;8(2):e55773. [Link] [DOI:10.1371/journal.pone.0055773]
15. Wang CH, Chang CC, Liang YM, Shih CM, Muggleton NG, Juan CH. Temporal preparation in athletes: a comparison of tennis players and swimmers with sedentary controls. J Mot Behav. 2013;45(1):55-63. [Link] [DOI:10.1080/00222895.2012.740522]
16. Ströhle A, Graetz B, Scheel M, Wittmann A, Feller C, Heinz A, et al. The acute antipanic and anxiolytic activity of aerobic exercise in patients with panic disorder and healthy control subjects. J Psychiatry Res. 2009;43(12):1013-7. [Link] [DOI:10.1016/j.jpsychires.2009.02.004]
17. Bandelow B, Broocks A, Pekrun G, George A, Meyer T, Pralle L, et al. The use of the panic and agoraphobia scale (P & A) in a controlled clinical trial. Pharmacopsychiatry. 2000;33(5):174-81. [Link] [DOI:10.1055/s-2000-12982]
18. da Silva GS, Unsain N, Mascó DH, Toscano-Silva M, de Amorim HA, Silva Araújo BH, et al. Early exercise promotes positive hippocampal plasticity and improves spatial memory in the adult life of rats. Hippocampus. 2012;22(2):347-58. [Link] [DOI:10.1002/hipo.20903]
19. Kamijo K, Pontifex MB, O'Leary KC, Scudder MR, Wu C. Castelli DM, et al. The effects of an afterschool physical activity program on working memory in preadolescent children. Development Sci. 2011;14(5):1046-58. [Link] [DOI:10.1111/j.1467-7687.2011.01054.x]
20. Hutton CP. Synergistic effects of diet and exercise on hippocampal function in chronically stressed mice. Neurosci. 2015;308:180-93. [Link] [DOI:10.1016/j.neuroscience.2015.09.005]
21. Sosso FA, Raouafi S. An overview of positive interaction between exercise and mental health. J Neurol Neurosci. 2017;8:215-9. [Link]
22. Burrel T. Circuit train your brain. N Sci. 2015;227(3035):32-7. [Link] [DOI:10.1016/S0262-4079(15)31032-0]