GMJ Medicine
eISSN : 2626-3041

Embase

Biosis Previews
description
Volume 3, Issue 3 (2024)
GMJM 2024, 3(3): 87-92 |
Back to browse issues page
Article Type:
Subject:





History
Received: 2023/12/8 | Accepted: 2024/06/15 | Published: 2024/07/22
Received: 2023/12/8 | Accepted: 2024/06/15 | Published: 2024/07/22
How to cite this article
Safa M, Tabarsi P, Ghassem Boroujerdi F, Hajizadeh F, Mirabzadeh Ardekani B. Evaluation and Comparison of the Cognitive Distortions of Tubercular Patients and Healthy People. GMJM 2024; 3 (3) :87-92
URL: http://gmedicine.de/article-2-241-en.html
URL: http://gmedicine.de/article-2-241-en.html
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



Rights and permissions
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:

1- Clinical Tuberculosis and Epidemiology Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- Mycobacteriology Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran
3- Chronic Respiratory Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- Massih Daneshvari Hospital, Tehran, Iran
5- Shahid Beheshti University of Medical Sciences, Tehran, Iran
2- Mycobacteriology Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran
3- Chronic Respiratory Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran
4- Massih Daneshvari Hospital, Tehran, Iran
5- Shahid Beheshti University of Medical Sciences, Tehran, Iran
Keywords:
| Abstract (HTML) (1607 Views)
Full-Text: (819 Views)
Introduction
Infectious or transmissible disease is a disease that is transmitted by infection and causes the incidence of disease symptoms. Meanwhile, tuberculosis is a common infectious disease that is caused by various mycobacterium species [1]. Currently, more than 20 million people in the world are infected with tuberculosis. Tuberculosis disease causes about two million deaths in the world, and it has been mentioned as a global emergency by the World Health Organization [2, 3]. Tuberculosis symptoms include hemoptysis, pain, fever and sweating at night, weight loss, and fatigue [4]. Our own country, Iran, is in serious danger of a tuberculosis outbreak because it is in the neighborhood of Pakistan and Afghanistan countries, which are among the most infected areas with tuberculosis bacteria in the world. Tuberculosis disease is most common in the Sistan & Baluchestan and the Golestan States of Iran. Iran has ranked as the 17th country for the outbreak of tuberculosis disease in the world. The incidence rate of tuberculosis disease is 26 in every 100,000 people in Iran, and 17.9% of the population is infected [5, 6]. On the other hand, tuberculosis disease is correlated with increased population, insufficient nutrition, and poverty in general. Pulmonary chronic diseases, smoking, alcoholism, and diabetes mellitus disease are among the risk factors for the incidence of tuberculosis disease. The most dangerous risk factor for tuberculosis disease in the world is Human Immunodeficiency Virus (HIV) [7-10]. Social stigma and isolation, disruption of interpersonal and social relationships, long-term treatment, decreased income, and psychological complications like depressive and anxiety disorders, as well as physical problems, are among the serious difficulties of tubercular patients [11]. Understanding the discrimination and stigma resulting from the disease plays an important role in the patient's experience of his or her illness. The rejection of tubercular patients by society, their isolated maintenance because of the contagiousness of the tuberculosis disease, and becoming a byword in society affect the mental health of tubercular patients in the long period and cause dramatic psychological complications [12]. The difficulties of tuberculosis disease are special painful experiences in the psychological, social, and biological life of the person, where the related stress plays an important role in the appearance of psychological problems [13].
According to the cognitive model, we always evaluate and interpret the information within our internal and external world. Our brains always classify the data and try to make sense of the environmental stimuli. The process of making sense includes some carelessness because the optimal mode of our knowledge and cognition is just the approximate representation of objective experiences. Thus, interpreting the surrounding environment is not a precise and objective process and is not completely in accordance with reality. Instead, it is distorted and accordant to active schemas of the people, alongside cognitive distortions or mistakes [14].
According to Aaron Beck's theory, some logical mistakes exist in the automatic thoughts and cognitions of people with affective and emotional disorders [15]. Special psychological statuses like mood, anxiety, and emotional disorders affect the way that the person encounters self and the world, which constitute distorted cognitions [14]. The primary shock of receiving the tuberculosis diagnosis usually results in a denial process for a long period of time, which may produce cognitive distortions about the disease. Negative impressions of tubercular patients about the self and the disease, the impressions of the society about the tuberculosis disease, the social beliefs about community health, and the society's dominant culture altogether play important roles in the social and mental status of the patient [13]. In fact, cognitive distortions are incorrect assumptions that result in thought bias. The thought bias would create distance between the person and the reality of life. It results in some misunderstandings in personal and interpersonal behaviors, which would make the person prone to psychiatric disorders. When the information processing is incorrect, cognitive distortions show up. Usually, people's important beliefs and schemas are exposed to cognitive distortions [15].
Some cognitive distortions include personalization, labeling, should statements, emotional reasoning, magnification and minimization, mental filter, overgeneralization, all-or-nothing thinking, fortune telling, catastrophizing, blaming, unfair comparison, always being regretful, and judging [16]. Cognitive distortions are among the psychological constructs of tubercular patients in encountering the disease and play a significant role in adherence to treatment and pulmonary rehabilitation [17]. The psychological adaptation of the tubercular patients is primarily impressed by negative impressions about the self. On the other hand, the attitude and understanding of the society about the tuberculosis disease is an important factor that can affect the understanding of the patient about the self [13].
According to the effects that the tuberculosis disease leaves on the life, physical and mental status, understanding, and thoughts of the patients, and due to the correlation of the psychiatric disorders with cognitive distortions and irrational beliefs, the goal of the current study was to identification and comparing the cognitive distortions of tubercular patients with healthy people for providing better and more comprehensive treatment for everyone. Indeed, psychological concepts are among the most important factors for adherence to treatment and pulmonary rehabilitation. The research hypothesis included the difference in cognitive distortions between tubercular patients and healthy people and the existence of more cognitive distortions in patients compared to the healthy group. In fact, the importance and necessity of the research are applied to providing precise and sufficient psychological services by achieving knowledge about the cognitive distortions of tubercular patients.
The early psychological and psychiatric interventions would improve the physical and psychological status and, eventually, quality of life. Considering and recognizing the psychological features of the patients, including cognitive distortions of the patients, which affect the disease and treatment process, helps the psychologists and psychiatrists to provide the treatment plan accordant with the patients' special characteristics and needs and ultimately obtain better treatment.
Materials and Methods
This was a case-control study in which cognitive distortions of tubercular patients and healthy people (hospital personnel) were compared. The proportion of tuberculosis disease in Iran is 26 out of every 100,000 people. Thus, the sample size could be 40 persons in each group, considering the confidence level of 1.96. However, we investigated 100 people in each group to reduce the error rate [18].
The sample groups were selected after the research project was confirmed by the research and ethical committee. The sampling process was done using a random method from the tuberculosis clinic and healthy personnel of a hospital in Tehran, Iran.
Essential information about the research was presented to the sample groups. After obtaining informed consent from the sample groups, the questioning process began.
The sample groups were assured that their information would be completely confidential and would be applied just as an article in general format. The study's statistical population included the hospital's tubercular patients and healthy personnel, where the work was done in the years 2015-2016.
The inclusion criteria for tubercular patients are the minimum age of 18, the absence of a psychiatric disorder that would cause psychiatric drug consumption by psychiatrist order, the ability to understand and answer the questions, complete consciousness, informed consent for participation in the study, and a definite diagnosis of tuberculosis disease.
The exclusion criteria for tubercular patients are the incidence of any physical problem interfering with the questioning process, the subject's reluctance to continue participating in the study, and loss of consciousness.The inclusion criteria for a healthy sample are working in the hospital, absence of psychiatric disorder that would cause psychiatric drug consumption by psychiatrist order, and
inclination to participate in the research.
The exclusion criteria of healthy subjects: reluctance to continue participating in the study.
Instruments
Demographic questionnaires evaluated age, gender, marital status, occupation, and education level.
The cognitive distortions scale includes 20 phrases that evaluate cognitive distortions that Albert Ellis introduced. The sub-scales of the cognitive distortions scale include all-or-nothing thinking, overgeneralization, mental filter, minimizing the positive, fortune telling, magnification and minimization, emotional reasoning, should statements, labeling, and personalization. The scoring is in Likert format, from 1 to 5. The person who uses more cognitive distortions receives a lower score, and vice versa. The Cronbach-Alpha for the internal consistency of the scale was 0.8. The validity coefficient of the scale was 0.85 [19].
Statistical analysis
Calculating the frequency, percentage, mean, standard deviation, and distribution tables were applied as descriptive statistics for data analysis. The inferential statistical methods, including t-test and two-way ANOVA, were applied to compare the mean scores in two groups and the cognitive distortions sub-scales and gender, respectively. The SPSS 22 software was used for data analysis.
Findings
The mean age of all 200 subjects was 39.94 years old. 43% were women and 57% were men. 32.5% were single, 62.5% were married, and 5% were divorced and widowed.14% had an elementary education degree, 13.5% had an intermediate education degree, 33.5% had a high school education degree, and 39% had an academic education degree. 53% had low-income jobs, 44.5% had mediocre-income jobs, and 2.5% had high-income jobs. There was a significant difference (p<0.001) in gender, education, and occupation status between the two groups. Number of men was significantly higher in tubercular patients group. The healthy group had a significantly higher education level compared to tubercular patients. The tubercular patients had significantly more jobs with low incomes. The two groups did not significantly differ in age and marital status.
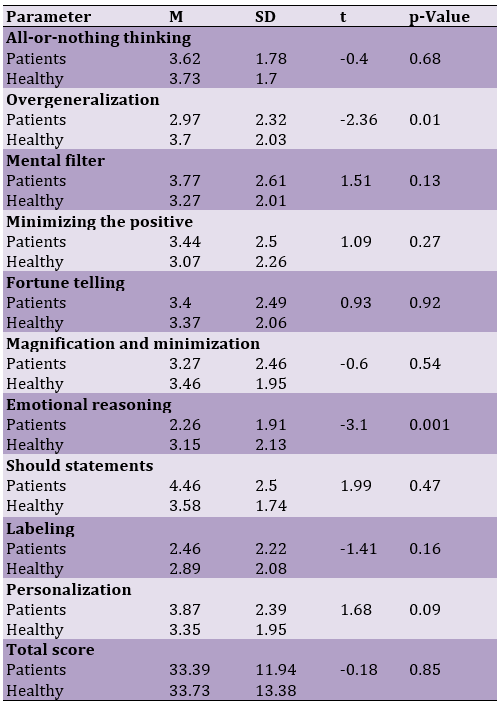
There were significant differences between the two groups in overgeneralization and emotional reasoning sub-scales (p<0.001). Tubercular patients used the mentioned sub-scales significantly more than healthy people. In addition, all-or-nothing thinking, magnification and minimization, and labeling cognitive distortions were more common in patients than in healthy people. The cognitive distortions of minimizing the mental filter were more common in the healthy group (Table 1).
Table 1. The comparison of cognitive distortions sub-scales in tubercular patient and healthy personnel groups by independent t-test
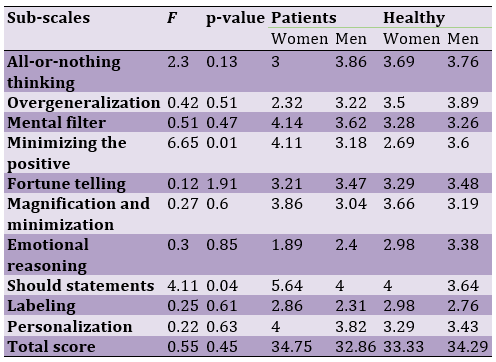
Female patients used cognitive distortions to minimize the positive and negative statements significantly less than others. Furthermore, women patients applied cognitive distortions related to emotional reasoning and overgeneralization more than others. The male patients used labeling cognitive distortions more than others (Table 2).
Table 2. Comparing the cognitive distortions sub-scales between patient and healthy men and women by two-way ANOVA
Discussion
The mean age of the tubercular patient was 40.69 years. 63.2% of them were men, and 57% of them were married. 39.1% had a high school education, and 69% had low-income jobs. In the current research, tubercular patients used more cognitive distortions. They specially applied overgeneralization and emotional reasoning cognitive distortions significantly more than others, manifesting exaggeration in disease symptoms and non-compliance of the patients to the physician's medical orders. In addition, cognitive distortions of magnification minimization and labeling were more common in patients than in healthy people. Minimizing the positive and mental filter cognitive distortions was more common in healthy people, which reflects insufficient attention to different subjects. Men used to minimize the positive and should statements significantly more than others, which shows the inflexibility of the men. Women patients used emotional reasoning and overgeneralization more than others, showing the characteristics of attributing to the self and exaggerating the problems. Male patients also used labeling cognitive distortion more than others.
We evaluate some other research in a similar domain to our current one. In a cross-sectional study on tubercular patients at Massih Daneshvari Hospital in Tehran, it was shown that tuberculosis disease would affect different aspects of the quality of life of the patients more than we expected. In the same vein, the most effects of tuberculosis disease are imposed on physical and mood status [20]. Yet, there is limited information about the quality of life of tubercular patients and the long-term effects of tuberculosis disease. Thus, systematic evaluation of the quality of life of tubercular patients in a more comprehensive style is essential [21]. Tubercular patients show various reactions when they receive the disease diagnosis. They may suffer depression, jealousy, fear, grudge, anger, feeling lonely, inefficiency, guilt, and suicidal ideation. However, suicide attempts are rare among them [13]. Various and severe psychiatric disorders exist in tubercular patients [22]. Psychological distress and psychosis symptoms have a high prevalence among tubercular patients [23]. 31% of them suffer from psychiatric disorders. Recognizing the psychiatric disorders in the primary stages of tuberculosis disease would help the patients in treatment compliance and improvement. Thus, referring the tubercular patients to psychiatrists and psychologists by other physicians should be developed more [16]. According to DSM-IV, some psychiatric disorders have been diagnosed in tubercular patients, which include: 1 - adjustment disorder, 2 - mood disorders (especially major depression, which is equivalent to depressive disorders in DSM-5), 3 - anxiety disorder (especially generalized anxiety disorder, acute stress disorder, post-traumatic stress disorder (equivalent to trauma and stressor-related disorders in DSM-5), 5 - delirium and other cognitive disorders.24 Meanwhile, major depression disorder, post-traumatic stress disorder, and acute stress disorder are among the most common psychiatric disorders in tuberculosis patients. In a study, major depression disorder was the most common psychiatric disorder in tubercular patients. Thus, evaluation of the mental health of the tubercular patients was recommended for comprehensive health care [25]. It was also indicated that depression and anxiety symptoms are important risk factors for a decrease in quality of life. They may cause impairment in the quality function, exacerbation of disease symptoms, long-term and frequent hospitalizations, failure to quit smoking, non-compliance with physical and rehabilitation treatments, and higher mortality rates [26]. Depression and anxiety symptoms impact the quality of life and other related factors more than other factors in chronic obstructive pulmonary patients [27]. Tubercular patients with anxiety and depression disorders understand the disease more than others [28]. Moreover, there is a correlation between low educational levels and psychological problems in tubercular patients [29]. There is also a significant correlation between marital conflicts with interpersonal cognitive distortions, dysfunctional attitudes, and irrational beliefs [30]. The hope factor and applying eclectic psychotherapies focused on hope significantly reduce unrealistic interpersonal expectations and cognitive distortions of couples [31]. Indeed, tubercular patients need to receive psychotherapy as well as physical treatment. Psychotherapies increase hopefulness, which is a determinant factor against tuberculosis disease [32].
One of the most important limitations of the research was the inappropriateness of the physical status of the patients, which made the questioning process so complicated and time-consuming. However, all of the questioners tried to interview the patients at the most appropriate time and place. In the future, it is suggested that the researchers evaluate various psychological variables in different organic patients to better recognize the patients and provide comprehensive treatment for them.
Conclusion
Considering the existence of two cognitive distortions in tubercular patients compared to healthy people, the current research depicts the necessity of paying attention to psychological factors in organic patients. Otherwise, the comprehensive treatment of the patients and, eventually, their improvement would be prevented.
Acknowledgments: None declared by the authors.
Ethical Permission: The current scientific research project has been approved by Massih Daneshvari Hospital's ethical committee. All participants gave informed consent, and the project was confirmed as conforming to the Declaration of Helsinki.
Conflicts of Interests: None declared by the authors.
Funding/Support: There was no funding source for the current article.
Infectious or transmissible disease is a disease that is transmitted by infection and causes the incidence of disease symptoms. Meanwhile, tuberculosis is a common infectious disease that is caused by various mycobacterium species [1]. Currently, more than 20 million people in the world are infected with tuberculosis. Tuberculosis disease causes about two million deaths in the world, and it has been mentioned as a global emergency by the World Health Organization [2, 3]. Tuberculosis symptoms include hemoptysis, pain, fever and sweating at night, weight loss, and fatigue [4]. Our own country, Iran, is in serious danger of a tuberculosis outbreak because it is in the neighborhood of Pakistan and Afghanistan countries, which are among the most infected areas with tuberculosis bacteria in the world. Tuberculosis disease is most common in the Sistan & Baluchestan and the Golestan States of Iran. Iran has ranked as the 17th country for the outbreak of tuberculosis disease in the world. The incidence rate of tuberculosis disease is 26 in every 100,000 people in Iran, and 17.9% of the population is infected [5, 6]. On the other hand, tuberculosis disease is correlated with increased population, insufficient nutrition, and poverty in general. Pulmonary chronic diseases, smoking, alcoholism, and diabetes mellitus disease are among the risk factors for the incidence of tuberculosis disease. The most dangerous risk factor for tuberculosis disease in the world is Human Immunodeficiency Virus (HIV) [7-10]. Social stigma and isolation, disruption of interpersonal and social relationships, long-term treatment, decreased income, and psychological complications like depressive and anxiety disorders, as well as physical problems, are among the serious difficulties of tubercular patients [11]. Understanding the discrimination and stigma resulting from the disease plays an important role in the patient's experience of his or her illness. The rejection of tubercular patients by society, their isolated maintenance because of the contagiousness of the tuberculosis disease, and becoming a byword in society affect the mental health of tubercular patients in the long period and cause dramatic psychological complications [12]. The difficulties of tuberculosis disease are special painful experiences in the psychological, social, and biological life of the person, where the related stress plays an important role in the appearance of psychological problems [13].
According to the cognitive model, we always evaluate and interpret the information within our internal and external world. Our brains always classify the data and try to make sense of the environmental stimuli. The process of making sense includes some carelessness because the optimal mode of our knowledge and cognition is just the approximate representation of objective experiences. Thus, interpreting the surrounding environment is not a precise and objective process and is not completely in accordance with reality. Instead, it is distorted and accordant to active schemas of the people, alongside cognitive distortions or mistakes [14].
According to Aaron Beck's theory, some logical mistakes exist in the automatic thoughts and cognitions of people with affective and emotional disorders [15]. Special psychological statuses like mood, anxiety, and emotional disorders affect the way that the person encounters self and the world, which constitute distorted cognitions [14]. The primary shock of receiving the tuberculosis diagnosis usually results in a denial process for a long period of time, which may produce cognitive distortions about the disease. Negative impressions of tubercular patients about the self and the disease, the impressions of the society about the tuberculosis disease, the social beliefs about community health, and the society's dominant culture altogether play important roles in the social and mental status of the patient [13]. In fact, cognitive distortions are incorrect assumptions that result in thought bias. The thought bias would create distance between the person and the reality of life. It results in some misunderstandings in personal and interpersonal behaviors, which would make the person prone to psychiatric disorders. When the information processing is incorrect, cognitive distortions show up. Usually, people's important beliefs and schemas are exposed to cognitive distortions [15].
Some cognitive distortions include personalization, labeling, should statements, emotional reasoning, magnification and minimization, mental filter, overgeneralization, all-or-nothing thinking, fortune telling, catastrophizing, blaming, unfair comparison, always being regretful, and judging [16]. Cognitive distortions are among the psychological constructs of tubercular patients in encountering the disease and play a significant role in adherence to treatment and pulmonary rehabilitation [17]. The psychological adaptation of the tubercular patients is primarily impressed by negative impressions about the self. On the other hand, the attitude and understanding of the society about the tuberculosis disease is an important factor that can affect the understanding of the patient about the self [13].
According to the effects that the tuberculosis disease leaves on the life, physical and mental status, understanding, and thoughts of the patients, and due to the correlation of the psychiatric disorders with cognitive distortions and irrational beliefs, the goal of the current study was to identification and comparing the cognitive distortions of tubercular patients with healthy people for providing better and more comprehensive treatment for everyone. Indeed, psychological concepts are among the most important factors for adherence to treatment and pulmonary rehabilitation. The research hypothesis included the difference in cognitive distortions between tubercular patients and healthy people and the existence of more cognitive distortions in patients compared to the healthy group. In fact, the importance and necessity of the research are applied to providing precise and sufficient psychological services by achieving knowledge about the cognitive distortions of tubercular patients.
The early psychological and psychiatric interventions would improve the physical and psychological status and, eventually, quality of life. Considering and recognizing the psychological features of the patients, including cognitive distortions of the patients, which affect the disease and treatment process, helps the psychologists and psychiatrists to provide the treatment plan accordant with the patients' special characteristics and needs and ultimately obtain better treatment.
Materials and Methods
This was a case-control study in which cognitive distortions of tubercular patients and healthy people (hospital personnel) were compared. The proportion of tuberculosis disease in Iran is 26 out of every 100,000 people. Thus, the sample size could be 40 persons in each group, considering the confidence level of 1.96. However, we investigated 100 people in each group to reduce the error rate [18].
The sample groups were selected after the research project was confirmed by the research and ethical committee. The sampling process was done using a random method from the tuberculosis clinic and healthy personnel of a hospital in Tehran, Iran.
Essential information about the research was presented to the sample groups. After obtaining informed consent from the sample groups, the questioning process began.
The sample groups were assured that their information would be completely confidential and would be applied just as an article in general format. The study's statistical population included the hospital's tubercular patients and healthy personnel, where the work was done in the years 2015-2016.
The inclusion criteria for tubercular patients are the minimum age of 18, the absence of a psychiatric disorder that would cause psychiatric drug consumption by psychiatrist order, the ability to understand and answer the questions, complete consciousness, informed consent for participation in the study, and a definite diagnosis of tuberculosis disease.
The exclusion criteria for tubercular patients are the incidence of any physical problem interfering with the questioning process, the subject's reluctance to continue participating in the study, and loss of consciousness.The inclusion criteria for a healthy sample are working in the hospital, absence of psychiatric disorder that would cause psychiatric drug consumption by psychiatrist order, and
inclination to participate in the research.
The exclusion criteria of healthy subjects: reluctance to continue participating in the study.
Instruments
Demographic questionnaires evaluated age, gender, marital status, occupation, and education level.
The cognitive distortions scale includes 20 phrases that evaluate cognitive distortions that Albert Ellis introduced. The sub-scales of the cognitive distortions scale include all-or-nothing thinking, overgeneralization, mental filter, minimizing the positive, fortune telling, magnification and minimization, emotional reasoning, should statements, labeling, and personalization. The scoring is in Likert format, from 1 to 5. The person who uses more cognitive distortions receives a lower score, and vice versa. The Cronbach-Alpha for the internal consistency of the scale was 0.8. The validity coefficient of the scale was 0.85 [19].
Statistical analysis
Calculating the frequency, percentage, mean, standard deviation, and distribution tables were applied as descriptive statistics for data analysis. The inferential statistical methods, including t-test and two-way ANOVA, were applied to compare the mean scores in two groups and the cognitive distortions sub-scales and gender, respectively. The SPSS 22 software was used for data analysis.
Findings
The mean age of all 200 subjects was 39.94 years old. 43% were women and 57% were men. 32.5% were single, 62.5% were married, and 5% were divorced and widowed.14% had an elementary education degree, 13.5% had an intermediate education degree, 33.5% had a high school education degree, and 39% had an academic education degree. 53% had low-income jobs, 44.5% had mediocre-income jobs, and 2.5% had high-income jobs. There was a significant difference (p<0.001) in gender, education, and occupation status between the two groups. Number of men was significantly higher in tubercular patients group. The healthy group had a significantly higher education level compared to tubercular patients. The tubercular patients had significantly more jobs with low incomes. The two groups did not significantly differ in age and marital status.
There were significant differences between the two groups in overgeneralization and emotional reasoning sub-scales (p<0.001). Tubercular patients used the mentioned sub-scales significantly more than healthy people. In addition, all-or-nothing thinking, magnification and minimization, and labeling cognitive distortions were more common in patients than in healthy people. The cognitive distortions of minimizing the mental filter were more common in the healthy group (Table 1).
Table 1. The comparison of cognitive distortions sub-scales in tubercular patient and healthy personnel groups by independent t-test
Female patients used cognitive distortions to minimize the positive and negative statements significantly less than others. Furthermore, women patients applied cognitive distortions related to emotional reasoning and overgeneralization more than others. The male patients used labeling cognitive distortions more than others (Table 2).
Table 2. Comparing the cognitive distortions sub-scales between patient and healthy men and women by two-way ANOVA
Discussion
The mean age of the tubercular patient was 40.69 years. 63.2% of them were men, and 57% of them were married. 39.1% had a high school education, and 69% had low-income jobs. In the current research, tubercular patients used more cognitive distortions. They specially applied overgeneralization and emotional reasoning cognitive distortions significantly more than others, manifesting exaggeration in disease symptoms and non-compliance of the patients to the physician's medical orders. In addition, cognitive distortions of magnification minimization and labeling were more common in patients than in healthy people. Minimizing the positive and mental filter cognitive distortions was more common in healthy people, which reflects insufficient attention to different subjects. Men used to minimize the positive and should statements significantly more than others, which shows the inflexibility of the men. Women patients used emotional reasoning and overgeneralization more than others, showing the characteristics of attributing to the self and exaggerating the problems. Male patients also used labeling cognitive distortion more than others.
We evaluate some other research in a similar domain to our current one. In a cross-sectional study on tubercular patients at Massih Daneshvari Hospital in Tehran, it was shown that tuberculosis disease would affect different aspects of the quality of life of the patients more than we expected. In the same vein, the most effects of tuberculosis disease are imposed on physical and mood status [20]. Yet, there is limited information about the quality of life of tubercular patients and the long-term effects of tuberculosis disease. Thus, systematic evaluation of the quality of life of tubercular patients in a more comprehensive style is essential [21]. Tubercular patients show various reactions when they receive the disease diagnosis. They may suffer depression, jealousy, fear, grudge, anger, feeling lonely, inefficiency, guilt, and suicidal ideation. However, suicide attempts are rare among them [13]. Various and severe psychiatric disorders exist in tubercular patients [22]. Psychological distress and psychosis symptoms have a high prevalence among tubercular patients [23]. 31% of them suffer from psychiatric disorders. Recognizing the psychiatric disorders in the primary stages of tuberculosis disease would help the patients in treatment compliance and improvement. Thus, referring the tubercular patients to psychiatrists and psychologists by other physicians should be developed more [16]. According to DSM-IV, some psychiatric disorders have been diagnosed in tubercular patients, which include: 1 - adjustment disorder, 2 - mood disorders (especially major depression, which is equivalent to depressive disorders in DSM-5), 3 - anxiety disorder (especially generalized anxiety disorder, acute stress disorder, post-traumatic stress disorder (equivalent to trauma and stressor-related disorders in DSM-5), 5 - delirium and other cognitive disorders.24 Meanwhile, major depression disorder, post-traumatic stress disorder, and acute stress disorder are among the most common psychiatric disorders in tuberculosis patients. In a study, major depression disorder was the most common psychiatric disorder in tubercular patients. Thus, evaluation of the mental health of the tubercular patients was recommended for comprehensive health care [25]. It was also indicated that depression and anxiety symptoms are important risk factors for a decrease in quality of life. They may cause impairment in the quality function, exacerbation of disease symptoms, long-term and frequent hospitalizations, failure to quit smoking, non-compliance with physical and rehabilitation treatments, and higher mortality rates [26]. Depression and anxiety symptoms impact the quality of life and other related factors more than other factors in chronic obstructive pulmonary patients [27]. Tubercular patients with anxiety and depression disorders understand the disease more than others [28]. Moreover, there is a correlation between low educational levels and psychological problems in tubercular patients [29]. There is also a significant correlation between marital conflicts with interpersonal cognitive distortions, dysfunctional attitudes, and irrational beliefs [30]. The hope factor and applying eclectic psychotherapies focused on hope significantly reduce unrealistic interpersonal expectations and cognitive distortions of couples [31]. Indeed, tubercular patients need to receive psychotherapy as well as physical treatment. Psychotherapies increase hopefulness, which is a determinant factor against tuberculosis disease [32].
One of the most important limitations of the research was the inappropriateness of the physical status of the patients, which made the questioning process so complicated and time-consuming. However, all of the questioners tried to interview the patients at the most appropriate time and place. In the future, it is suggested that the researchers evaluate various psychological variables in different organic patients to better recognize the patients and provide comprehensive treatment for them.
Conclusion
Considering the existence of two cognitive distortions in tubercular patients compared to healthy people, the current research depicts the necessity of paying attention to psychological factors in organic patients. Otherwise, the comprehensive treatment of the patients and, eventually, their improvement would be prevented.
Acknowledgments: None declared by the authors.
Ethical Permission: The current scientific research project has been approved by Massih Daneshvari Hospital's ethical committee. All participants gave informed consent, and the project was confirmed as conforming to the Declaration of Helsinki.
Conflicts of Interests: None declared by the authors.
Funding/Support: There was no funding source for the current article.
References
1. Kumar V, Abbas AK, Fausto N, Mitchell RN. Robbins basic pathology. Saunders Elsevier. 2007;7(2):516-22. [Link]
2. Mirhaghani L, Nasehi M. National tuberculosis control guideline. Tehran: Andishmand; 2009. [Persian] [Link]
3. Paul A, Denise G, Renee R, Sidibe K. The guideline for the prevention of tuberculosis. Tehran: Andishmand; 2009. [Link]
4. Robabi H, Navidian A, Pishkar Mofrad Z. Quality of life of patients with pulmonary tuberculosis during treatment course. J Mazandaran Univ Me Sci (JMUMS). 2012;22(93):104-13. [Link]
5. Alavi SM, Sefidgaran G, Karami F. Comparative study on knowledge about tuberculosis in two cities with different tuberculosis epidemiological index in Khuzestan, 2004. Scient Med J (AJUMS). 2009;8(1):63-9. [Persian] [Link]
6. Jadgal KM, Zareban I, Alizadeh-Siuki H, Izadirad H. The impact of educational intervention based on health belief model on promoting self-care behaviors in patients with smear-positive pulmonary TB. J. Health Educ. Health Promo Summ. 2014;2(2):143-52. [Persian] [Link]
7. Lawn S, Zumla A. Seminar tuberculosis. Lancet. 2011;378(9785):57-72. [Link] [DOI:10.1016/S0140-6736(10)62173-3]
8. Restrepo BI. Convergence of the tuberculosis and diabetes epidemics: Renewal of old acquaintances. Clin Infect Dis. 2007;45(4):436-8. [Link] [DOI:10.1086/519939]
9. van Zyl Smit R, Pai M, Yew W, Leung CC, Zumla A, Bateman ED, et al. Global lung health: The colliding epidemics of tuberculosis, tobacco smoking, HIV and COPD. Eur Resp J. 2010;35(1):27-33. [Link] [DOI:10.1183/09031936.00072909]
10. Organization WH. The sixteenth global report on tuberculosis. Tuberculosis: Executive summary. WHO Rep. 2011;2011:1-2. [Link]
11. Hansel NN, Wu AW, Chang B, Diette GB. Quality of life in tuberculosis: Patient and provider perspectives. Quality Life Res. 2004;(3):639-52. [Link] [DOI:10.1023/B:QURE.0000021317.12945.f0]
12. Guo N, Marra F, Marra CA. Measuring health-related quality of life in tuberculosis: A systematic review. Health Quality Of Life Outcomes. 2009;7(1):14. [Link] [DOI:10.1186/1477-7525-7-14]
13. Ndoro T. Attitudes and perceptions towards TB in Grahamstown East in a time of HIV/AIDS. 2009. [Link]
14. Mootabi FFL. On becoming a cognitive behavioral therapist. Tehran: Danjeh; 2013. [Persian] [Link]
15. Wright JH, Brown GK, Thase ME, Basco MR. Learning cognitive-behavior therapy: An illustrated guide. Washington: Amer Psychiatric Pub;2017. [Link] [DOI:10.1176/appi.books.9781615374823]
16. Islam AT, Hussain M, Siddique MA, Badruddoza SM. Pattern of psychiatric illness among tuberculosis patients. Anwer Khan Mod Med Coll J. 2015;6(2):25-9. [Link] [DOI:10.3329/akmmcj.v6i2.31589]
17. Harrison SL. Exploring patients' perceptions following an acute exacerbation of chronic obstructive pulmonary disease to inform tailored strategies to enhance pulmonary rehabilitation, School of Psychology; 2014. [Link] [DOI:10.2147/COPD.S41938]
18. Shahab Jahanloo A. Step-by-step guide to medical and health research. Tehran: Darya; 2010. [Link]
19. Jelokhanian M, Khademi A. Effectiveness of cognitive distortion training on marital satisfaction in women of Behzisty's counseling centers. J Modern Psychol Res. 2013;8(29):89-111. [Persian] [Link]
20. Darvish PurKakhki AEZ, Mir Saeidi ZSM, Masjedi MR, Velayati AA. Evaluation of the quality of life of the tubercular patients referring to Massih Daneshvari Hospital in the year 2005. Iran J Infect Dis Trop Med. 2006;11(32):49-56. [Persian] [Link]
21. Brown J, Capocci S, Smith C, Morris S, Abubakar I, Lipman M. Health status and quality of life in tuberculosis. Int J Infect Dis. 2015;32:68-75. [Link] [DOI:10.1016/j.ijid.2014.12.045]
22. Theron G, Peter J, Zijenah L, Chanda D, Mangu C, Clowes P, et al. Psychological distress and its relationship with non-adherence to TB treatment: A multicentre study. BMC Infect Dis. 2015;15(1):253. [Link] [DOI:10.1186/s12879-015-0964-2]
23. Lasebikan V, Ige O. Prevalence of psychosis in tuberculosis patients and their nontuberculosis family contacts in a multidrug treatment-resistant treatment center in Nigeria. Gen Hosp Psych. 2015;37(6):542-7. [Link] [DOI:10.1016/j.genhosppsych.2015.05.012]
24. Pachi A, Bratis D, Moussas G, Tselebis A. Psychiatric morbidity and other factors affecting treatment adherence in pulmonary tuberculosis patients. Tubercul Res Treat. 2013;2013:489865. [Link] [DOI:10.1155/2013/489865]
25. Srivastava AS, Ramdinee NA, Matah S, Tripathi MN, Pandit B, Yadav JS. Psychiatric morbidities in patients with pulmonary tuberculosis. Dysphrenia. 2014;5(2). [Link]
26. Hammonds TL. The influence of the caregiver on healthcare outcomes in patients with chronic obstructive pulmonary disease (COPD) [dissertation]. Kent: Kent State University; 2015. [Link]
27. Gado O, Basiony L, Ibrahim M, Shady I, Affara N. Anxiety-depressive symptoms in patients with chronic obstructive pulmonary disease (COPD) and impact on outcome. J Depress Anxiety. 2015;4(2):1-6. [Link]
28. Galhenage J, Rupasinghe J, Abeywardena G, De Silva A, Williams S, Gunasena B. Psychological morbidity and illness perception among patients receiving treatment for tuberculosis in a tertiary care centre in Sri Lanka. Ceylon Med J. 2016;61(1):37-40. [Link] [DOI:10.4038/cmj.v61i1.8261]
29. Aghanwa H, Erhabor GE. Demographic/socioeconomic factors in mental disorders associated with tuberculosis in southwest Nigeria. J Psychosom Res. 1998;45(4):353-60. [Link] [DOI:10.1016/S0022-3999(98)00006-3]
30. Ebrahimi A, Zeinodini SS, Merasi MR. The association between psychopathology of family relationships and cognitive vulnerability (Dysfunctional attitude and interpersonal cognitive distortion). J Isfahan Med School. 2012;29(167):2390-9. [Persian] [Link]
31. Bahari F, Fatehizadeh M, Ahmadi S, Molavi H, Bahrami F. The effect of hope, forgiveness and combined marital counseling on interpersonal cognitive distortions of divorcing couples. Behav Sci Res. 2010;8(1):25-33. [Persian] [Link] [DOI:10.1037/e537902012-137]
32. Safa M, Ebrahimi M, Ghassem Boroujerdi F, Talischi F. Cognitive group psychotherapy in patients with tuberculosis. Pract Clin Psychol. 2013;1(3):157-62. [Link]